Professional Documents
Culture Documents
Effect of Nicotine On Vasoconstrictor and Vasodilator Responses in Human Skin Vasculature
Uploaded by
Paul CoevOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Effect of Nicotine On Vasoconstrictor and Vasodilator Responses in Human Skin Vasculature
Uploaded by
Paul CoevCopyright:
Available Formats
Am J Physiol Regulatory Integrative Comp Physiol
281: R1097–R1104, 2001.
Effect of nicotine on vasoconstrictor and vasodilator
responses in human skin vasculature
CLAIRE E. BLACK,1,2 NING HUANG,1 PETER C. NELIGAN,1,2 RONALD H. LEVINE,1,2
JOAN E. LIPA,1,2 STEVEN LINTLOP,3 CHRISTOPHER R. FORREST,1,2 AND CHO Y. PANG1,2,4
1
Research Institute, The Hospital for Sick Children, and Departments of 2Surgery and 4Physiology,
University of Toronto, and 3Center of Forensic Sciences, Toronto, Ontario M5G 1X8, Canada
Received 14 December 2000; accepted in final form 4 June 2001
Black, Claire E., Ning Huang, Peter C. Neligan, Ro- some time (16, 21, 31, 38, 43). More recently, there is
nald H. Levine, Joan E. Lipa, Steven Lintlop, Christo- also the clinical impression that cigarette smoking
pher R. Forrest, and Cho Y. Pang. Effect of nicotine on increases the incidence of skin ischemic necrosis in
vasoconstrictor and vasodilator responses in human skin skin flap surgery (45). This clinical impression is sup-
vasculature. Am J Physiol Regulatory Integrative Comp
ported by the observations that cigarette smoke inten-
Physiol 281: R1097–R1104, 2001.—Our objective was to test
the hypothesis that acute exposure of human skin vascula- sified skin ischemic necrosis in skin flap surgery in the
ture to nicotine may have deleterious effects on endothelial rat and hamster (11, 23, 28, 42). Skin vasospasm asso-
function. Vasoconstriction and vasorelaxation in isolated per- ciated with cigarette smoking and or use of smokeless
fused human skin flaps (⬃8 ⫻ 18 cm) derived from dermoli- tobacco implies that the by-products of tobacco may
pectomy specimens were assessed by studying changes in have detrimental effects on the skin vasculature, re-
skin perfusion pressure measured by a pressure transducer, sulting in reduction in skin circulation, but the mech-
and skin perfusion was assessed by a dermofluorometry anism is unclear. Epidemiological studies on the dele-
technique (n ⫽ 4 or 5). It was observed that nicotine (10⫺7 M) terious effects of cigarette smoking in humans
amplified (P ⬍ 0.05) the norepinephrine (NE)-induced con- indicated that the risk in developing cigarette smok-
centration-dependent (10⫺7-10⫺5 M) increase in skin vaso-
ing-related cardiovascular disease was related to the
constriction compared with the control. This amplification
effect of nicotine in NE-induced skin vasoconstriction was not nicotine content of the cigarette (2, 3, 18). Therefore,
blocked by the nicotine-receptor antagonist hexamethonium much of the research on the pathogenesis of cigarette
(10⫺6 M) or the cyclooxygenase inhibitor indomethacin (10⫺5 smoking-related cardiovascular diseases has been fo-
M). It was also observed that ACh and nitroglycerin (NTG) cused on the deleterious effect of nicotine on the vas-
elicited a concentration-dependent (10⫺8-10⫺5 M) vasorelax- culature. To date, there is experimental evidence to
ation in skin flaps preconstricted with 8 ⫻ 10⫺7 M of NE. The indicate that chronic nicotine treatment has deleteri-
vasorelaxation induced by ACh was attenuated (P ⬍ 0.05) in ous effects on the hemodynamics of the cardiovascular
the presence of nicotine (10⫺7 M) compared with the control. system either by causing direct injury to the blood
However, skin vasorelaxation induced by NTG was not af- vessel wall (8, 19, 54) or by modulating the synthesis
fected by nicotine (10⫺7 M). ACh and NTG are known to
and/or release of vasoactive neurohumoral substances
induce endothelium-dependent and -independent vasorelax-
ation, respectively. The present findings were interpreted to (1, 49, 50) to promote vasospasm and platelet aggrega-
indicate that acute exposure of human skin vasculature to tion.
nicotine was associated with 1) amplification of NE-induced Of particular interest to us is the effect of nicotine on
skin vasoconstriction and 2) impairment of endothelium- skin circulation. With the use of skin flap models, we
dependent skin vasorelaxation. Cyclooxygenase products and have demonstrated that chronic nicotine treatment in
nicotine receptors blocked by hexamethonium were not in- rats and pigs (13–15) mimicked the deleterious effect
volved in the amplification of NE-induced skin vasoconstric- of cigarette smoke in increasing the extent of skin
tion by nicotine. These findings may provide further insight ischemic necrosis in skin flap surgery in the rat and
into the pathogenesis of skin vasospasm in skin flap surgery hamster (11, 23, 28, 42). This deleterious effect was
and skin ischemic disease associated with cigarette smoking
associated with an increase in skin flap content of
or use of smokeless tobacco.
norepinephrine (NE) and a decrease in skin flap blood
norepinephrine; acetylcholine; nitroglycerin flow (13–15). More recently, it has been reported by
other investigators that acute nicotine treatment selec-
tively potentiated NE-induced arteriole contraction in
THE ASSOCIATION OF CIGARETTE smoking or use of smoke- the hamster cheek pouch. This potentiation effect was
less tobacco (e.g., chewing tobacco) with arterioscle- attributed to the nicotine-induced impairment of endo-
rotic peripheral vascular disease and thromboangiitis thelial function in the arterioles (33). Most recently, it
obliterans (Buerger’s disease) has been identified for
The costs of publication of this article were defrayed in part by the
Address for reprint requests and other correspondence: C. Y. Pang, payment of page charges. The article must therefore be hereby
The Hospital for Sick Children, 555 Univ. Ave., Toronto, Ontario marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734
M5G 1X8, Canada (E-mail: pang@sickkids.on.ca). solely to indicate this fact.
http://www.ajpregu.org 0363-6119/01 $5.00 Copyright © 2001 the American Physiological Society R1097
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
R1098 NICOTINE AND ENDOTHELIAL FUNCTION
has been demonstrated that acute nicotine treatment Skin Perfusion Technique
mimicked the cigarette smoking-induced endothelial The skin flap with its cannulated arterial and venous
dysfunction in the human dorsal hand vein. Specifi- perforator was placed on an aluminum mesh stand and was
cally, local or transdermal administration of nicotine at subsequently connected to the commercially available MX
a dose reproducing plasma concentration observed dur- Amber perfuser apparatus (model Two-Ten; MX Interna-
ing cigarette smoking impaired endothelium-depen- tional, Aurora, CO). The perfusate consisted of modified
dent vasodilation in human dorsal hand veins (9, 47). Krebs-Henseleit buffer with the following composition (in
All these recent findings may have important implica- mM): 100 NaCl, 4.60 KCl, 1.10 NaH2PO4⫺, 1.20 MgSO42⫺, 2.25
tions for the direct vascular effect of nicotine, which CaCl2, 30 NaHCO3⫺, and 13 glucose. BSA (Cohen fraction V)
was added to the buffer for a final concentration of 6.5%. The
contributes to the pathogenesis of vasospasm in skin
buffer was then stirred and filtered (Whatman no. 40) and
ischemic disease and in skin flap surgery. To our equilibrated within the reservoir chamber of the perfusion
knowledge, no studies have been conducted to examine apparatus with 95% O2 and 5% CO2 at 37 ⫾ 0.1°C, pH 7.40 ⫾
the effect of nicotine on skin vascular function, espe- 0.03 mmHg, and PO2 450 ⫾ 16 mmHg. The PO2 of the
cially in human skin vasculature. Therefore, the objec- perfusate collected at the venous outflow was 180 ⫾ 25
tive of this project was to test the hypothesis that mmHg. This observation indicated adequate supply of oxy-
nicotine may have deleterious effects on the endothe- gen to the skin flap as there was minimal arteriovenous
lial function in human skin vasculature. To this end, shunt flow (⬍1%) in this skin flap model (27). An adjustable-
we used the established isolated perfused human skin rate pump (model 7014; Cole-Parmer Instrument, Vernon
Hills, IL) was used to deliver perfusate, which passed
flap model (25, 26, 32) to investigate the local effect of through a bubble trap in the reservoir to the arterial catheter
nicotine on vasoconstrictor and vasodilator responses of the skin flap. A three-way connector linked the tubing from
in human skin vasculature. the pump to the flap and allowed for parallel connection of a
pressure transducer (AB high-performance pressure trans-
MATERIALS AND METHODS ducer; Data Instruments, Lexington, MA). The transducer
output continuously displayed the perfusion pressure on a
Source of Human Skin Specimens digital monitor (Trandicator II 621A digital strain gauge;
Doric Scientific, San Diego, CA) and a chart recorder (Linea-
The abdominal pannus excised from patients undergoing corder WR 3101; Graphtec).
dermolipectomy serves no purpose to the patient and is The buffer flow rate was adjusted (2.0 ⫾ 0.4 ml/min) to
normally disposed of by incineration. A clinical protocol was achieve a stable baseline perfusion pressure of 45–50 mmHg.
approved for the design of skin flaps (⬃8 ⫻ 18 cm) from the A baseline of ⬃50 mmHg was chosen because results from
excised pannus for in vitro skin perfusion experiments. At previous studies with this human skin flap model revealed it
the end of each experiment, the skin specimen was returned to provide good tissue perfusion with minimal leakage and
to the Department of Pathology for incineration in the nor- edema formation of less than 10% water retention (25, 32). In
mal manner. addition, it has been estimated that a perfusion pressure of
The median age of the patients was 44 yr (range 26–65 yr), 50 mmHg, when Krebs buffer with an albumin concentration
and all these patients were female. The skin specimens of 65 g/l is used, is equivalent to the perfusion pressure of
accepted for this project did not have scars, lesions, or infec- ⬃90 mmHg in a whole blood perfusion (4). A perfusion
tion, and the patients were not known to smoke cigarettes or pressure of 50 mmHg with a similar perfusate was also
to have any systemic disease. successfully used in studies of the more aerobically active
isolated perfused cat hindlimb (53).
Skin Flap Model and Cannulation Technique A 45-min stabilization period was allowed at the beginning
for In Vitro Skin Perfusion of each experiment. The surface temperature (⬃34°C) of the
skin flap was monitored using a thermistor probe (YS1 series
The anatomy and design of the human skin flap model 400; Yellow Springs Instruments, Yellow Springs, OH) con-
used in the present studies were described by us previously nected to a microcomputer thermometer (Series 084202;
(32). This skin flap model resembled clinical skin free flaps Cole-Parmer Instrument). Drugs were infused intra-arteri-
used for reconstructive surgery. This skin flap model has ally through a sidearm port driven by a separate pump of
been validated and studied with various kinds of vasodilator adjustable rates (model P-1; Pharmacia LKB). Under the
and vasoconstrictor drugs (25, 26, 32). constant flow condition in which the pump rate remained
The width and length of this skin flap model were ⬃8 ⫻ 18 constant, a change in perfusion pressure in response to drug
cm, respectively. The vascular pedicle in the proximal end of administration is indicative of a change in vascular resis-
the skin flap consisted of a paired perforator artery and vein tance of the skin flap. The change in perfusion pressure
(0.5- to 1.5-mm diameter), which were cannulated with 22- or induced by drug treatment in each skin flap was standard-
24-gauge angiocatheter, depending on vessel size. Perfusion ized by its baseline perfusion pressure and is expressed as a
buffer containing 10 U/ml of heparin was gently instilled percentage of baseline perfusion pressure.
through the arterial angiocather with a 3-ml syringe until Criteria for Rejection of Skin Flap
venous outflow was observed, thus confirming that the vas-
culature of the skin flap was satisfactory for an in vitro A skin flap was deemed to be vascularly reactive if it
perfusion experiment. All perfusion experiments in the demonstrated a concentration-dependent increase in perfu-
present studies were initiated within 2 h of excision of skin sion pressure to NE. At the end of the last dose of NE in each
specimens. It was previously demonstrated that the skin flap experiment, ACh (10⫺5 M) was used to test endothelium-
was thereafter metabolically and physiologically stable for at dependent relaxation. Finally, 0.2 ml of fluorescein dye (20
least 5 h of in vitro perfusion (26). mg) was infused into each flap to characterize the area of skin
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
NICOTINE AND ENDOTHELIAL FUNCTION R1099
perfusion. Any skin flap that did not respond to the concen- vation of skin vasoconstriction assessed by measurement of
tration-dependent vasoconstrictor effect of NE and vasodila- perfusion pressure in the preceding study. Specifically, the
tor effect of ACh and showed ⬍6-cm length in dye stain NE-induced (8 ⫻ 10⫺7 M) decrease in dermal perfusion in
(perfusion) was not included in this study. isolated perfused human skin flaps was assessed in the
absence and presence of 10⫺7 M of nicotine, using the der-
Surface Dermofluorometry Technique for Assessment mofluorometry technique. Total dye fluorescence was as-
of Skin Perfusion in Isolated Perfused Skin Flaps sessed at the end of: the stabilization period (baseline); 15-
min infusion of vehicle; and 15-min infusion of NE in the
The dermofluorometry technique for indirect assessment
absence and presence of 10⫺7 M of nicotine.
of in vivo dermal perfusion has been validated against the
radioactive microsphere technique in the pig (51). Dermoflu- Protocol 3: to investigate the role of nicotine receptors and
orometry has also been applied to the present isolated per- endogenous cyclooxygenase products in the effect of nicotine
fused human skin flap model in vitro (24, 25, 32). In the on NE-induced skin vasoconstriction in isolated perfused
present study, dermofluorometry was used to corroborate the human skin. The effect of nicotine (10⫺7 M) on the cumula-
observation of skin vasoconstriction assessed by measure- tive concentration-dependent vasoconstrictor effect of NE on
ment of perfusion pressure. Specifically, confluent circles of skin perfusion pressure was studied in the absence and
1-cm diameter were marked along the longitudinal midline of presence of the nicotine-receptor antagonist hexamethonium
the skin flap surface. After a 45-min stabilization period, the (10⫺6 M). Hexamethonium infusion was started 45 min be-
background fluorescence in each circular skin area was mea- fore nicotine infusion and followed by NE infusion 45 min
sured (fluorescence unit) using a dermofluorometer (Fluore- later.
scan Unit; Santa Barbara Technology, Santa Barbara, CA). In a separate study, all skin flaps were pretreated with
Fluorescein dye with a final concentration of 3 ⫻ 10⫺5 M was 10⫺5 M of indomethacin. The vasoconstrictor effect of NE
then infused into the skin flap for 4 min, and fluorescence in (8 ⫻ 10⫺7 M) on skin perfusion pressure was studied in the
each circular area was measured again. A washout period of absence and presence of 10⫺7 M of nicotine. Infusion of
15 min was allowed, and the background fluorescence was indomethacin and nicotine was started 45 min before NE
taken again. After the perfusion pressure had stabilized infusion.
subsequent to drug infusion for study of skin vascular reac- Protocol 4: to investigate the effect of nicotine on ACh- or
tivity, fluorescein dye infusion was repeated, and skin fluo- nitroglycerin-induced vasorelaxation in isolated perfused hu-
rescence was measured again. The difference in fluorescence man skin. The effect of nicotine (10⫺7 M) on cumulative
units for each circular skin area between the background and concentration-dependent vasorelaxation induced by ACh or
postfluorescein dye infusion was defined as the net fluores- nitroglycerin (NTG) was studied in isolated perfused human
cence units for that area. The total dye fluorescence is the skin flaps preconstricted with 8 ⫻ 10⫺7 M of NE. ACh and
sum of all net fluorescence units measured from all circular NTG were used in this study because it is well known that
skin areas along the midline of the skin flap. ACh elicits endothelium-dependent vasorelaxation and NTG
elicits endothelium-independent vasorelaxation (35–37).
Biochemicals
All reagents and drugs were purchased from Sigma Chem- Statistics
ical (Oakville, Ontario) except the following: NE from SABEX
All values are expressed as means ⫾ SE. The number of
Pharmaceutical (Boucherville, Quebec) and fluorescein dye
(fluorescein sodium 10%) from Dioptic Laboratories observations and the specific statistical test used in each
(Markham, Ontario). study are indicated in the legend of each figure. The level of
Indomethacin, a cyclooxygenase inhibitor, was dissolved in significance for all tests was set at Pⱕ 0.05.
200 l ethanol before mixing with buffer solution. This con-
centration of alcohol did not affect the baseline perfusion RESULTS
pressure. Other drugs used in the present studies were
dissolved in buffer. Purified water (Milli-Q Water System, Effect of Nicotine on NE-Induced Skin
Bedford, MA) was used for making perfusion buffer. Fresh Vasoconstriction Assessed by Perfusion Pressure in
perfusion buffer and drug solutions were made on the day of Isolated Perfused Human Skin Flaps
experiment. The drugs were stored at 4°C before use.
Intra-arterial infusion of nicotine (10⫺7 M) was
Experimental Protocols started 45 min before infusion of NE in the isolated
Protocol 1: to investigate the effect of nicotine on NE-
perfused human skin flap. Infusion of nicotine alone
induced skin vasoconstriction by assessment of perfusion did not have any effect on the baseline perfusion pres-
pressure in isolated perfused human skin. Cumulative con- sure. The baseline perfusion pressures before (47.6 ⫾
centration-dependent (10⫺7-10⫺5 M) vasoconstrictor effects 1.7 mmHg) and after (48.3 ⫾ 1.0 mmHg) nicotine
of NE on skin perfusion pressure were studied in the absence infusion were not significantly different.
and presence of 10⫺7 M nicotine in isolated human skin flaps NE elicited an increase in perfusion pressure in
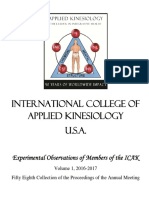
perfused with a constant flow rate of Krebs buffer. NE was isolated perfused human skin flaps in a concentration-
used in this study because it was reported that nicotine dependent (10⫺8–10⫺5 M) manner (Fig. 1). This in-
selectively potentiated the vasoconstrictor effect of NE in
hamster cheek pouch arterioles (33).
crease in skin perfusion pressure induced by NE was
Protocol 2: to investigate the effect of nicotine on NE- significantly higher (P ⬍ 0.05) in the presence of 10⫺7
induced skin vasoconstriction by assessment of skin perfusion M of nicotine compared with the control, thus indicat-
in isolated perfused human skin. Skin perfusion was assessed ing that nicotine amplified the skin vasoconstrictor
by the dermofluorometry technique to corroborate the obser- effect of NE.
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
R1100 NICOTINE AND ENDOTHELIAL FUNCTION
Fig. 3. Role of nicotine receptors in the effect of nicotine (10⫺7 M) on
NE-induced skin vasoconstriction. Values are means ⫾ SE, n ⫽ 4.
Fig. 1. Effect of nicotine (10⫺7 M) on norepinephrine (NE)-induced The cumulative concentration-dependent increase in perfusion elic-
skin vasoconstriction. Values are means ⫾ SE, n ⫽ 4. The cumula- ited by NE and nicotine was not significantly different in the pres-
tive concentration-dependent increase in perfusion pressure elicited ence or absence of the nicotine-receptor antagonist hexamethonium
by NE in isolated perfused human skin flaps was significantly higher (10⫺6 M); analysis of variance with repeated measures.
in the presence of nicotine compared with the control; analysis of
variance with repeated measures, P ⬍ 0.05.
Role of Nicotine Receptors and Endogenous
Cyclooxygenase Products in Effect of Nicotine on NE-
Effect of Nicotine on NE-Induced Skin Induced Vasoconstriction in Isolated Perfused Human
Vasoconstriction Assessed by Dermofluorometry Skin Flaps
Technique in Isolated Perfused Human Skin Flaps
In the preceding study, it was observed that the
The amplification effect of nicotine on NE-induced NE-induced increase in skin perfusion pressure in hu-
vasoconstriction was further assessed by using the man skin was significantly (P ⬍ 0.05) higher in the
dermofluorometry technique. The total dye fluores- presence of 10⫺7 M of nicotine compared with the
cence in the vehicle-treated skin flaps was similar to control (Fig. 1). Here, it was observed that the increase
the baseline perfusion (100 ⫾ 4%). Infusion of 8 ⫻ 10⫺7 in skin perfusion pressure induced by combined NE
M of NE significantly (P ⬍ 0.05) reduced the total dye and nicotine was similar in skin flaps with or without
fluorescence to 37 ⫾ 4% (P ⬍ 0.05) of the control pretreatment with the nicotine-receptor antagonist
hexamethonium (10⫺6 M) (Fig. 3). Therefore, nicotine
(vehicle). In the presence of 10⫺7 M of nicotine, this
receptors blocked by hexamethonium were not in-
same concentration of NE further reduced the total
volved in the amplification effect of nicotine in NE-
fluorescence to 20 ⫾ 5% (P ⬍ 0.05) of the control (Fig. induced increase in perfusion pressure.
2). Thus the present results from the dermofluorom- In a separate study, all skin flaps were pretreated
etry study supported the observation from the preced- with indomethacin (10⫺5 M). It was observed that the
ing study that nicotine amplified the skin vasoconstric- NE-induced increase in perfusion pressure was still
tor effect of NE by assessment of perfusion pressure. significantly (P ⬍ 0.05) higher in the presence of 10⫺7
M of nicotine compared with NE alone (Fig. 4). This
observation is interpreted to indicate that the endoge-
nous cyclooxygenase products were not involved in the
Fig. 2. Effect of nicotine (10⫺7 M) on NE-induced (8 ⫻ 10⫺7 M)
decrease in dermal perfusion. Dermal perfusion was assessed by
measuring the total dye fluorescence in the skin flap using a der- Fig. 4. Role of cyclooxygenase products in the effect of nicotine (10⫺7
mofluorometry technique. Total dye fluorescence is expressed as a M) on NE-induced skin vasoconstriction. Values are means ⫾ SE,
percentage of the control baseline before drug treatment. Values are n ⫽ 4. All isolated perfused skin flaps were pretreated with the
means ⫾ SE, n ⫽ 4. Means without a common letter are significantly cyclooxygenase inhibitor indomethacin (10⫺5 M). The increase in
different (a ⬎ b ⬎ c); 1-way analysis of variance followed by Duncan’s perfusion pressure induced by NE and nicotine was significantly
multiple range test for comparison of means, P ⬍ 0.05. higher than NE alone; Mann-Whitney U test, P ⬍ 0.05.
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
NICOTINE AND ENDOTHELIAL FUNCTION R1101
amplification effect of nicotine on NE-induced increase
in perfusion pressure.
Effect of Nicotine on ACh- and NTG-Induced
Vasorelaxation in Isolated Perfused Human Skin
Flaps Preconstricted with NE
ACh elicited a concentration-dependent relaxation in
isolated perfused human skin flaps preconstricted with
8 ⫻ 10⫺7 M of NE (Fig. 5). The concentration-depen-
dent vasorelaxation induced by ACh in isolated per-
fused human skin flaps preconstricted with NE was
significantly (P ⬍ 0.05) reduced in the presence of 10⫺7
M of nicotine compared with the control (Fig. 5). Fig. 6. Effect of nicotine (10⫺7 M) on cumulative concentration-
NTG also elicited a concentration-dependent vasore- dependent vasorelaxation of nitroglycerin in isolateral perfused hu-
laxation in isolated perfused human skin flaps precon- man skin flap preconstricted with 8 ⫻ 10⫺7 M of NE. Vasorelaxation
stricted with 8 ⫻ 10⫺7 M of NE. However, the concen- is expressed as a percentage of contraction to 8 ⫻ 10⫺7 M of NE.
Values are means ⫾ SE, n ⫽ 5. The vasorelaxation induced by
tration-dependent vasorelaxation induced by NTG in nitroglycerin was not significantly different in the presence or ab-
human skin flaps preconstricted with 8 ⫻ 10⫺7 M of NE sence of nicotine; analysis of variance with repeated measures.
was not significantly different in the absence or pres-
ence of 10⫺7 M of nicotine (Fig. 6).
impair the endothelial vasorelaxation function in the
DISCUSSION
vasculature.
Major Findings in the Present Studies
Levels of Nicotine and NE Used for the Study
We used the isolated perfused human skin flap of Endothelial Function
model to investigate the acute local effect of nicotine on
Studies on nicotine pharmacokinetics in cigarette
vasoconstrictor and vasodilator responses in human
smokers have shown that peak levels of plasma nico-
skin vasculature. We observed that 1) nicotine ampli-
tine range from ⬃30 to 50 ng/ml (7, 12). The half-life of
fied the concentration-dependent skin vasoconstrictor
plasma nicotine due to metabolism is ⬃2.2 h (12). It
effect of NE; 2) nicotine attenuated endothelium-de-
has also been reported that most cigarette smokers
pendent skin vasorelaxation induced by ACh in NE-
tend to modify their smoking behavior (e.g., depth of
preconstricted skin vasculature; 3) nicotine did not
puffing or inhalation, and frequency of smoking) to
affect the endothelium-independent vasorelaxation in-
maintain fairly constant plasma levels of nicotine (12).
duced by NTG in NE-preconstricted skin vasculature;
The average peak plasma levels of nicotine in smoke-
and 4) cyclooxygenase products and nicotine receptors
less tobacco users have also been reported to range
blocked by hexamethonium were not involved in the
from ⬃22 to 30 ng/ml (17). The level of nicotine in the
amplification of NE-induced skin vasoconstriction by
perfusion buffer used in the present studies was 10⫺7
nicotine. These observations led us to speculate that
M (16.2 ng/ml), which is well within the range of
exposure of human skin vasculature to nicotine may
plasma levels of nicotine in cigarette smokers and
users of smokeless tobacco.
We previously observed that NE elicited concentra-
tion-dependent skin vasoconstriction over a range of
10⫺7–10⫺5 M in isolated perfused pig skin flaps (44).
The mean concentration of NE required to produce
half-maximal increase in perfusion pressure (EC50)
was 1.1 ⫻ 10⫺6 M. Similar results were reported by
other investigators for isolated perfused pig skin flaps
(46). In addition, the skin contents of NE in rat and pig
skin flaps were also in the range of 10⫺7–10⫺6 M (15,
22). Therefore, 10⫺7- to 10⫺5-M concentrations of NE
were used for the present studies.
Experimental Model for the Study of Nicotine
on Vasoconstrictor and Vasodilator Responses
Fig. 5. Effect of nicotine (10⫺7 M) on cumulative concentration- in Human Skin Vasculature
dependent vasorelaxation induced by ACh in isolated perfused hu-
man skin flaps preconstricted with 8 ⫻ 10⫺7 M of NE. Vasorelaxation Many of the in vivo cardiovascular effects observed
is expressed as a percentage of contraction to 8 ⫻ 10⫺7 M of NE.
Values are means ⫾ SE, n ⫽ 5. The ACh-induced vasorelaxation was
after cigarette smoking, such as increases in blood
significantly reduced in the presence of nicotine compared with the pressure and heart rate, result from activation of the
control; analysis of variance with repeated measures, P ⬍ 0.05. sympathoadrenal system by nicotine (5, 6). Thus the
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
R1102 NICOTINE AND ENDOTHELIAL FUNCTION
net effect of nicotine on vascular tone is determined by Mechanism of Action of Nicotine in Vasoconstrictor
the balance between peripheral and central sites of and Vasodilator Responses in Human Skin
action of nicotine, and the local vascular effect of nico- Vasculature
tine cannot be distinguished. Recently, the human
We previously observed in isolated perfused pig skin
dorsal hand vein model was used to study the acute
flaps that NE-induced concentration-dependent vaso-
local effect of nicotine on vascular endothelial function
constriction was enhanced in the presence of the nitric
with minimal systemic effect. Specifically, physiologi- oxide synthase (NOS) inhibitor NG-nitro-L-arginine
cal saline with or without nicotine and/or vasoactive (L-NNA), and this skin vasoconstriction was further
drugs was infused continuously into a dorsal hand vein enhanced in the presence of both L-NNA and the cyclo-
to study the local vasoconstriction and vasorelaxation oxygenase inhibitor indomethacin (15). We also previ-
effects of these drugs by measuring the changes in ously observed that L-NNA attenuated the vasorelax-
diameters of the dorsal hand vein (9). So far, there is no ation effect of ACh in isolated perfused human skin
study on the local effect of nicotine on human skin flaps preconstricted with NE (25). These observations
vasculature relevant to vasospasm in skin ischemic were interpreted to indicate that the endothelium of
disease and in skin flap surgery. Our isolated perfused skin vasculature could be stimulated to synthesize
human skin flap model permitted local intra-arterial and/or release vasorelaxing factors such as NO and
infusion of nicotine and drugs into the skin vasculature prostacyclin (PGI2) to counteract the vasoconstrictor
to study local vasoconstrictor and vasodilator re- effect of NE or to mediate the vasorelaxation effect of
sponses (26, 32). Krebs buffer instead of whole blood ACh. Experimental evidence from other laboratories is
was used for perfusate in the present studies so that also available to indicate that contractions of isolated
the local effect of nicotine on endothelial function could blood vessels caused by NE or stimulation of adrener-
be investigated in the absence of blood cells and circu- gic nerves were associated with simultaneous release
lating neurohumoral vasoactive substances. of endothelium-derived NO and PGI2 (10, 48). The
mechanisms were not investigated in these studies.
Local Effect of Nicotine on Vasoconstrictor and However, it is known that NE activates ␣1-adrenocep-
Vasodilator Responses in Human Skin Vasculature tors in smooth muscle cells to cause vasoconstriction.
NE also activates ␣2-adrenoceptors in the endothelium
In the present studies, we have obtained evidence to to stimulate synthesis/release of NO and PGI2 (52).
indicate that nicotine amplified skin vasoconstriction ACh is also known to activate muscarinic receptors in
induced by NE. Specifically, NE-induced skin vasocon- the endothelium to stimulate synthesis/release of NO
striction assessed by perfusion pressure or dermal per- (52). These previous observations provide insight into
fusion was significantly increased in the presence of the mechanism of nicotine in amplification of NE-in-
10⫺7 M of nicotine compared with NE alone (Figs. 1 duced skin vasoconstriction (Fig. 1) and in attenuation
and 2). of ACh-induced vasorelaxation (Fig. 5) observed in
There is also evidence from the present studies to isolated perfused human skin flaps in the present stud-
indicate that nicotine amplified the NE-induced skin ies. Specifically, we speculate that nicotine might have
vasoconstriction independent of nicotine receptors inhibited the NOS activity in the endothelium to cause
blocked by hexamethonium and endogenous cyclooxy- a reduction in synthesis/release of NO in the endothe-
genase products. This interpretation is based on the lium. Therefore, there was less NO to counteract NE-
following observations. The nicotine-receptor antago- induced skin vasoconstriction or to mediate ACh-in-
nist hexamethonium did not attenuate the concentra- duced vasorelaxation. We further speculate that the
mechanism of action of nicotine did not involve hexa-
tion-dependent increase in perfusion pressure induced
methonium-sensitive receptors or cyclooxygenase
by combined NE and nicotine in isolated perfused hu-
products, because the amplification effect of nicotine on
man skin flaps (Fig. 3). Moreover, the cyclooxygenase
NE-induced skin vasoconstriction was not attenuated
inhibitor indomethacin did not block the amplification by hexamethonium or indomethacin (Figs. 3 and 4).
effect of nicotine in NE-induced increase in perfusion This line of reasoning may also explain why nicotine
pressure in isolated perfused human skin flaps (Fig. 4). did not affect the baseline perfusion pressure of iso-
Furthermore, we have also obtained evidence to in- lated perfused human skin flaps. Specifically, the de-
dicate that nicotine attenuated endothelium-depen- crease in NO synthesis due to inhibition of NOS activ-
dent but not endothelium-independent vasorelaxation ity in the endothelium by nicotine could have been
in human skin. Specifically, the concentration-depen- compensated by an increase in PGI2 synthesis at base-
dent vasorelaxation effect of ACh in isolated perfused line level; thus the baseline perfusion pressure re-
human skin flaps preconstricted with NE was signifi- mained unchanged. However, this small increase in
cantly reduced in the presence of 10⫺7 M of nicotine PGI2 synthesis could not compensate for the decrease
compared with ACh alone (Fig. 5). However, the same in NO synthesis in the endothelium caused by nicotine
nicotine treatment did not affect the concentration- in NE-induced skin vasoconstriction or in ACh-induced
dependent vasorelaxation induced by NTG in isolated vasorelaxation. There is in vivo evidence to support
perfused human skin flaps preconstricted with NE this speculation as well. Specifically, it has been re-
(Fig. 6). ported that a similar level of nicotine (14.0 ⫾ 1.6 ng/ml)
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
NICOTINE AND ENDOTHELIAL FUNCTION R1103
did not affect the baseline diameter of the hamster fied skin vasospasm induced by cigarette smoking in
cheek pouch arterioles, but this same level of nicotine skin flap surgery. However, we have also previously
potentiated the NE-induced vasoconstriction in the observed in rats that the detrimental effect of chronic
hamster cheek pouch in vivo (33, 34). nicotine treatment on skin flap blood flow and viability
was reversible and was not encountered when nicotine
Potential Limitations was withheld 2 wk before skin flap surgery (14). This
information may also be relevant to certain states of
It is important to point out that we only studied the
ischemic skin disease as it has been reported that
acute effect of nicotine on vasoconstrictor and vasodi-
resolution of symptoms such as skin vasospasm and
lator responses in NE-preconstricted human skin vas-
pain in Buerger’s disease (thromboangiitis obliterans)
culature. It is not known if these responses will also be
induced by use of tobacco could be achieved in some
seen in chronic nicotine treatment and/or with vaso-
patients by abstinence from tobacco use and a regimen
constrictors other than NE. There is evidence to indi-
of a vasodilating drug (20, 30, 40, 43).
cate that nicotine impaired ACh-induced endothelium-
In summary, we demonstrated for the first time that
dependent vasorelaxation in both acute and chronic
acute nicotine treatment amplified the skin vasocon-
nicotine treatment in hamster cheek pouch arterioles
strictor effect of NE and impaired the endothelium-
(35–37); thus there is evidence for us to speculate that
dependent vasorelaxation in isolated perfused human
the acute and chronic deleterious effect of nicotine on
skin flaps preconstricted with NE. Cyclooxygenase
endothelial function is similar. However, the amplifi-
products and nicotine receptors blocked by hexametho-
cation effect of nicotine on vasoconstriction in hamster
nium were not involved in the amplification of NE-
pouch arterioles seemed to be selective to NE (33).
induced skin vasoconstriction by nicotine. These obser-
So far, we have demonstrated that nicotine amplified
vations lent support to our hypothesis that nicotine
the vasoconstrictor effect of NE and impaired the ACh-
may have deleterious effects on endothelial function in
induced endothelium-dependent vasorelaxation in hu-
skin vasculature, but the mechanism has yet to be
man skin vasculature in vitro. These findings are in
investigated.
line with the in vivo observations reported by other
investigators that local administration of nicotine po- The authors thank D. Whitwell and D. McIntyre for typing this
tentiated the vasoconstrictor effect of NE (33) and manuscript.
impaired the endothelium-dependent vasorelaxation This research project was supported by an operating grant from
The Smokeless Tobacco Research Council (Grant 0784) and the
in hamster cheek pouch arterioles (35–37) and in hu- Canadian Institute of Health Research (Grant MOP-8048) to C. Y.
man dorsal hand veins (9, 47). However, it is unclear Pang.
why these vascular effects of nicotine were not ob-
served in tail artery ring segments and isolated per- REFERENCES
fused mesenteric vasculature obtained from rats with
1. Armitage AK. Effects of nicotine and tobacco smoke on blood
chronic nicotine treatment or in coronary artery seg- pressure and release of catecholamines from the adrenal glands.
ments obtained from dogs with chronic nicotine treat- Br J Pharmacol 25: 515–526, 1965.
ment (29, 39). The differences in these results could 2. Aronow WS and Swansen AJ. The effect of low-nicotine ciga-
reflect differences in vasculature, experimental design, rettes on angina pectoris. Ann Intern Med 71: 599–601, 1969.
3. Auerback O, Carter HW, Garfinkle L, and Hammond EC.
and levels of nicotine used. Cigarette smoking and coronary artery disease. Chest 70: 697–
705, 1976.
Perspectives 4. Avolio AP, Spain JAE, and Liard JD. Plasma protein concen-
tration and control of coronary vascular resistance in isolated rat
The effect of nicotine on amplification of NE-induced heart. Am J Physiol Heart Circ Physiol 238: H471–H480, 1980.
vasoconstriction and impairment of endothelium-de- 5. Benowitz NL. The role of nicotine in smoking-related cardio-
pendent vasorelaxation observed in human skin in the vascular diseases. Prev Med 26: 412–417, 1997.
6. Benowitz NL and Gourlay SG. Cardiovascular toxicity of
present studies may have important clinical implica- nicotine: implications for nicotine replacement therapy. J Am
tions in the pathogenesis of skin vasospasm in skin flap Coll Cardiol 29: 1422–1431, 1997.
surgery and skin ischemic disease. For example, there 7. Benowitz NL, Kuyt F, and Jacob P III. Circadian blood
is the clinical impression that cigarette smoking in- nicotine concentrations during cigarette smoking. Clin Pharma-
creases the incidence of skin ischemic necrosis in skin col Ther 32: 758–764, 1982.
8. Booyse FM, Ouikowicz G, and Quarfoot AJ. Effects of
flap surgery (45). We have previously demonstrated chronic oral consumption of nicotine on the rabbit aortic endo-
that chronic nicotine treatment in rats and pigs (13– thelium. Am J Pathol 102: 229–238, 1981.
15) mimicked the detrimental effect of cigarette smok- 9. Chalon S, Moreno H, Benowitz NL, Hoffman BB, and
ing in increasing the extent of skin flap ischemic ne- Blaschke TF. Nicotine impairs endothelium-dependent dilation
in human veins in vivo. Clin Pharmacol Ther 67: 391–397, 2000.
crosis, and this detrimental effect was associated with 10. Cohen R. Role of the endothelium in vascular adrenergic neu-
an increase in skin content of NE, presumably released rotransmission. In: Endothelial Regulation of Vascular Tone,
by nerve endings in the skin (15). Here, we demon- edited by Ryan US and Rubanyi GM. New York: Dekker, 1992, p.
strated for the first time in human skin that nicotine 155–169.
may also amplify the skin vasoconstrictor effect of NE, 11. Craig S and Rees TD. The effects of smoking on experimental
skin flaps in hamsters. Plast Reconstr Surg 75: 842–846, 1985.
probably by inhibition of NOS activity in the endothe- 12. Feyerabend C, Ings RMJ, and Russell MAH. Nicotine phar-
lium to reduce NO synthesis. Together, these observa- macokinetics and its application to intake from smoking. Br J
tions provide insight into the pathogenesis of intensi- Clin Pharmacol 19: 239–247, 1985.
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
R1104 NICOTINE AND ENDOTHELIAL FUNCTION
13. Forrest CR, Pang CY, and Lindsay WK. Dose and time 34. Mayhan WG and Patel KP. Effect of nicotine on endothelium-
effects of nicotine treatment on the capillary blood flow and dependent arteriolar dilation in vivo. Am J Physiol Heart Circ
viability of random pattern skin flaps in the rat. Br J Plast Surg Physiol 272: H2337–H2342, 1997.
40: 295–299, 1987. 35. Mayhan WG and Sharpe GM. Superoxide dismutase restores
14. Forrest CR, Pang CY, and Lindsay WK. Pathogenesis of endothelium-dependent arteriolar dilation during acute infusion
ischemic necrosis in random-pattern skin flaps induced by long- of nicotine. J Appl Physiol 85: 1292–1298, 1998.
term low-dose nicotine treatment. Plast Reconstr Surg 87: 518– 36. Mayhan WG and Sharpe GM. Chronic exposure to nicotine
528, 1991. alters endothelium-dependent arteriolar dilatation: effect of su-
15. Forrest CR, Xu N, and Pang CY. Evidence for nicotine-in- peroxide dismutase. J Appl Physiol 86: 1126–1134, 1999.
duced skin flap ischemic necrosis in the pig. Can J Physiol 37. Mayhan WG, Sharpe GM, and Anding P. Agonist-induced
Pharmacol 72: 30–38, 1994. release of nitric oxide during acute exposure nicotine. Life Sci 65:
16. Gifford RW and Hines EA. Complete clinical remission in 1829–1857, 1999.
thromboangiitis obliterans during abstinence from tobacco: re- 38. McKusick VA, Harris WS, Otteson OE, Goodman RM, Shel-
port of case. Proc Mayo Clinic 26: 241–245, 1951. ley WM, and Bloodwell RO. Burger’s disease: a distinct clin-
17. Gritz ER, Baer-Weiss V, Benowitz NL, Van Vunakis H, and ical and pathologic entity. JAMA 181: 5–12, 1962.
Jarvick ME. Plasma nicotine and cotinine concentration in 39. Miller VM, Clouse WD, Tonnessen BH, Boston US, Sever-
habitual smokeless tobacco users. Clin Pharmacol Ther 30: 201– son SR, Bonde S, Rud KS, and Hurt RD. Time and dose effect
209, 1981. of transdermal nicotine on endothelial function. Am J Physiol
18. Hill P and Wynder EL. Smoking and cardiovascular disease: Heart Circ Physiol 279: H1913–H1921, 2000.
effect of nicotine on the serum epinephrine and corticoids. Am 40. Mills JL and Proten JM. Buerger’s disease: a review and
Heart J 87: 491–496, 1974. update. Semin Vasc Surg 6: 14–23, 1993.
19. Hladove CJ. Endothelial injury by nicotine and its prevention. 41. Moreno H Jr, Chalon S, Urae A, Tangphao O, Abiose AK,
Experientia 35: 1585–1586, 1978. Hoffman BB, and Blaschke TF. Endothelial dysfunction in
20. Joyce JW. Buerger’s disease (thromboangiitis obliterans). human hand vein is rapidly reversible after smoking cessation.
Rheum Dis Clin North Am 16: 463–470, 1990. Am J Physiol Heart Circ Physiol 275: H1040–H1045, 1998.
21. Juergens JL, Barker NW, and Hines EA. Arteriosclerosis 42. Nolan J, Jenkins RA, Kurihara K, and Schultz R. The acute
obliterans: review of 520 cases with special reference to patho- effects of cigarette smoke exposure on experimental skin flaps.
genic and prognostic factors. Circulation 21: 188–195, 1960. Plast Reconstr Surg 75: 544–549, 1985.
22. Jurell G, Hjemdahl P, and Fredholm BB. On the mechanism 43. O’Dell JR, Linder J, Markin RS, and Moore GF. Thrombo-
by which antiadrenergic drugs increase survival of critical skin angiitis obliterans (Buerger’s disease) and smokeless tobacco.
Arthritis Rheum 30: 1054–1056, 1987.
flaps. Plast Reconstr Surg 72: 518–525, 1983.
44. Pang CY, Yang RZ, Neligan P, Xu N, Chin C, Zhong A, and
23. Kaufman T, Eihenlaub EH, Levine M, Hurwitz DJ, and
Forrest CR. Vascular effects and mechanisms of action of en-
Klain M. Tobacco smoking: importance of experimental flap
dothelium-1 in isolated perfused pig skin. J Appl Physiol 79:
survival. Ann Plast Surg 13: 468–472, 1984.
2106–2113, 1995.
24. Kreidstein ML, Levine RH, Knowlton RJ, and Pang CY.
45. Rees TD, Liverett DM, and Guy CI. The effect of cigarette
Serial fluorometric assessments of skin perfusion in isolated
smoking on skin flap survival in the face-lift patient. Plast
perfused human skin flaps. Br J Plast Surg 48: 288–293, 1995.
Reconstr Surg 73: 911–915, 1984.
25. Kreidstein MD, Pang CY, Carlsen LN, and Xu N. Evidence 46. Rogers RA and Riviere JE. Pharmacologic modulation of the
for endothelium-dependent and endothelium-independent vaso- cutaneous vasculature in the isolated perfused porcine skin flap.
dilation in human skin flaps. Can J Physiol Pharmacol 70: J Pharm Sci 83: 1682–1689, 1994.
1208–1216, 1992. 47. Sabha M, Tanus-Santos JE, Toledo JCY, Cittadino M,
26. Kreidstein ML, Pang CY, Levine RH, and Knowlton RJ. Rocha JC, and Moreno H. Transdermal nicotine mimics the
The isolated perfused human skin flap: design, perfusion tech- smoking-induced endothelial disfunction. Clin Pharmacol Ther
nique, metabolism and vascular reactivity. Plast Reconstr Surg 68: 167–174, 2000.
87: 741–749, 1991. 48. Segarra G, Medina P, Revert F, Masia S, Vila JM, Sucha L,
27. Kreidstein ML, Zacks SL, and Pang CY. Study of the micro- and Aldasoro M. Modulation of adrenergic contraction of dog
circulation in the isolated perfused human skin flap model. Surg pulmonary arteries by nitric oxide and prostacyclin. Gen Phar-
Forum 41: 664–666, 1990. macol 32: 583–589, 1999.
28. Lawrence WT, Murphy CR, Robson MC, and Hegger JP. 49. Seidler FJ and Slotkin TA. Effects of chronic nicotine admin-
The detrimental effect of cigarette smoking on flap survival: an istration on the denervated rat adrenal medulla. Br J Pharmacol
experimental study in the rat. Br J Plast Surg 37: 216–219, 56: 201–208, 1976.
1984. 50. Su C and Bevan JA. Blockade of the nicotine-induced norepi-
29. Li Z, Barrios V, Buchholz JN, Glenn TG, and Duckles SP. nephrine release by cocaine, phenoxybenzamine and desipri-
Chronic nicotine administration does not affect peripheral vas- mine. J Pharmacol Exp Ther 175: 533–540, 1970.
cular reactivity in the rat. J Pharmacol Exp Ther 271: 1135– 51. Thomson JG and Kerrigan CL. Dermofluorometry: thresh-
1142, 1994. olds for prediction flap survival. Plast Reconstr Surg 83: 859–
30. Lie JT. Thromboangiitis obliteran (Buerger’s disease) revisited. 864, 1989.
Pathol Annu 23: 257–291, 1988. 52. Vanhoutte PM. Endothelium dysfunction and vascular disease.
31. Lie JT. Thromboangiitis obliteran (Buerger’s disease) and In: Endothelium, Nitric Oxide and Atherosclerosis: From Basic
smokeless tobacco. Arthritis Rheum 31: 812–813, 1988. Mechanisms to Clinical Implications, edited by Panza JA and
32. Lipa JE, Neligan PC, Perreault TM, Baribeau J, Levine Cannon RO III. Armonk, NY: Futura, 1999, p. 79–96.
RH, Knowlton RJ, and Pang CY. Vasoconstrictor effect of 53. Watson PD. Colloid osmotic pressure changes in isolated iso-
endothelin-1 in human skin: role of ETA and ET receptors. Am J gravimetric cat hindlimb. Am J Physiol Heart Circ Physiol 242:
Physiol Heart Circ Physiol 276: H359–H367, 1999. H512–H519, 1982.
33. Mayhan WG. Acute infusion of nicotine potentiates norepineph- 54. Zimmerman M and McGeachie J. The effect of nicotine on
rine-induced vasoconstriction in the hamster cheek pouch. J Lab aortic endothelium: a quantitative ultrastructural study. Athero-
Clin Med 133: 48–54, 1999. sclerosis 63: 33–41, 1987.
AJP-Regulatory Integrative Comp Physiol • VOL 281 • OCTOBER 2001 • www.ajpregu.org
Downloaded from journals.physiology.org/journal/ajpregu (046.097.169.022) on June 2, 2021.
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- International College of Applied Kinesiology USA (PDFDrive)Document241 pagesInternational College of Applied Kinesiology USA (PDFDrive)dvenumohan100% (4)
- Part 5 Emergency Response PlanDocument23 pagesPart 5 Emergency Response Planalex.kollosovNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DC - M. Youssry Final WhiteDocument21 pagesDC - M. Youssry Final Whitemarwa abdelmegedNo ratings yet
- Self-Care PowerpointDocument17 pagesSelf-Care PowerpointJessa C. RamosNo ratings yet
- Imsbc CodeDocument4 pagesImsbc Codeabhimanyu6874No ratings yet
- Box 17 GAD Checlist For Project Monitoring and EvaluationDocument2 pagesBox 17 GAD Checlist For Project Monitoring and EvaluationRonnie ManaoNo ratings yet
- Tobacco-Associated Oral LesionsDocument48 pagesTobacco-Associated Oral LesionsSamridhi Srivastava100% (1)
- Chicken PoxDocument16 pagesChicken PoxAlbert TerbioNo ratings yet
- A Systematic Review and Meta-Analysis of The Prevalence and Predictors of Anemia Among Children in EthiopiaDocument15 pagesA Systematic Review and Meta-Analysis of The Prevalence and Predictors of Anemia Among Children in EthiopiaAura NirwanaNo ratings yet
- Ocp HukmDocument2 pagesOcp Hukmcac kepongNo ratings yet
- Safety Data Sheet: Product Name: Mobil Velocite Oil No. 10Document10 pagesSafety Data Sheet: Product Name: Mobil Velocite Oil No. 10Khoa HuynhNo ratings yet
- Organic Blueberries, 18 OzDocument5 pagesOrganic Blueberries, 18 OzJesse ManekNo ratings yet
- Grade 12 LFSC Informal Test Reproduction MemoDocument4 pagesGrade 12 LFSC Informal Test Reproduction Memomokgopofranklin75No ratings yet
- The Sympto-Thermal Method - Ten Years of Change PDFDocument18 pagesThe Sympto-Thermal Method - Ten Years of Change PDFFabian GuardaNo ratings yet
- English Research LUNA Group4Document30 pagesEnglish Research LUNA Group4ascnellapNo ratings yet
- The War On Drugs - An International EncyclopediaDocument368 pagesThe War On Drugs - An International EncyclopediaNintendo big NNo ratings yet
- Guide For Reflection Using Tanner's (2006) Clinical Judgment ModelDocument3 pagesGuide For Reflection Using Tanner's (2006) Clinical Judgment Modelapi-429421778No ratings yet
- Challenges For The Management of Emergency Care From The Perspective of NursesDocument9 pagesChallenges For The Management of Emergency Care From The Perspective of NursesEnis SpahiuNo ratings yet
- Aiims Dka ProtocolDocument9 pagesAiims Dka Protocolbbboghara100% (1)
- Comparison of Biogas Productivity in Thermophilic and Mesophilic Anaerobic Digestion of Bioethanol Liquid WasteDocument9 pagesComparison of Biogas Productivity in Thermophilic and Mesophilic Anaerobic Digestion of Bioethanol Liquid WasteKentner Chavez CorreaNo ratings yet
- 38 30 PBDocument8 pages38 30 PBMahusay Neil DominicNo ratings yet
- Mulluscum Contagiosum Cantharone Article PDFDocument6 pagesMulluscum Contagiosum Cantharone Article PDFmasjokoNo ratings yet
- Preparation #1 Divided PowdersDocument23 pagesPreparation #1 Divided PowdersIvy Rose OrozcoNo ratings yet
- Normal Reference Range Values in Adult Echocardiography F - 2016 - Indian HeartDocument2 pagesNormal Reference Range Values in Adult Echocardiography F - 2016 - Indian HeartBryan NguyenNo ratings yet
- Bioderma FinalDocument17 pagesBioderma FinalHậu PhúcNo ratings yet
- Chapter 4 - Mixed Venous Oxygen SaturationDocument3 pagesChapter 4 - Mixed Venous Oxygen SaturationJamesNo ratings yet
- THE Quality OF Life AND Caregiving Burden Among Caregivers OF People With Dementia IN Hanoi, BAC Ninh AND HAI Phong, VietnamDocument310 pagesTHE Quality OF Life AND Caregiving Burden Among Caregivers OF People With Dementia IN Hanoi, BAC Ninh AND HAI Phong, VietnamCHEE KOK SENGNo ratings yet
- Emergency Phone Number: 1-866-272-4378: Material Safety Data Sheet 6010 Welding ElectrodeDocument1 pageEmergency Phone Number: 1-866-272-4378: Material Safety Data Sheet 6010 Welding ElectrodeSona MahardhikaNo ratings yet
- Ob AssessmentDocument2 pagesOb AssessmentNathalie kate petallarNo ratings yet
- Room Temperature Stability of Drug Products Labeled For Refrigerated StorageDocument3 pagesRoom Temperature Stability of Drug Products Labeled For Refrigerated StorageAhmed YousefNo ratings yet