You might also like
- Project Azorian: The CIA and the Raising of the K-129From EverandProject Azorian: The CIA and the Raising of the K-129Rating: 4 out of 5 stars4/5 (17)
- Investigation of Fatal Accident on Offshore Oil RigDocument37 pagesInvestigation of Fatal Accident on Offshore Oil RigkfranovskyNo ratings yet
- Blowout Investigation Brazos Block 417 July 13, 2001Document43 pagesBlowout Investigation Brazos Block 417 July 13, 2001Dan MarrNo ratings yet
- Investigation of 2000 Offshore Oil Rig BlowoutDocument16 pagesInvestigation of 2000 Offshore Oil Rig BlowoutasdasdNo ratings yet
- f1020 - Teamwork and LeadershipDocument13 pagesf1020 - Teamwork and LeadershipAhmad Syarir AbdullahNo ratings yet
- Remembering The Ocean Ranger: Accident Investigation and Lessons LearnedDocument16 pagesRemembering The Ocean Ranger: Accident Investigation and Lessons Learnedchris100% (2)
- ReportDocument222 pagesReportgmcleod1977No ratings yet
- Pentlan: An Investigation Into The Grounding of The Dry CarrierDocument21 pagesPentlan: An Investigation Into The Grounding of The Dry CarrierLyubomir IvanovNo ratings yet
- From: - . - . - . - Sent: ToDocument9 pagesFrom: - . - . - . - Sent: ToCREWNo ratings yet
- Deepwater Horizon Oil SpillDocument24 pagesDeepwater Horizon Oil SpillRaymundo AlarconNo ratings yet
- Eerl 72-23 Project TugboatDocument219 pagesEerl 72-23 Project TugboatMisterSpacerockNo ratings yet
- Republic of The Marshall Islands DEEPWATER HORIZON Marine Casualty Investigation Report-High ResolutionDocument216 pagesRepublic of The Marshall Islands DEEPWATER HORIZON Marine Casualty Investigation Report-High Resolutiondan_mcgraw73No ratings yet
- Investigation Reportsuncor Altares PDFDocument12 pagesInvestigation Reportsuncor Altares PDFR GunalanNo ratings yet
- MMS Report on 2005 Capsizing of Chevron's Typhoon TLPDocument7 pagesMMS Report on 2005 Capsizing of Chevron's Typhoon TLPYANGRUYANNo ratings yet
- Goldch 4Document95 pagesGoldch 4heatherNo ratings yet
- fpso-USCG RequirementsDocument17 pagesfpso-USCG RequirementsAji VasudevanNo ratings yet
- New Orleans Environmental News - Articles About The BP Oil Spill For Examiner - Com (July 2010 - Present)Document29 pagesNew Orleans Environmental News - Articles About The BP Oil Spill For Examiner - Com (July 2010 - Present)Laurie Diane LeonardNo ratings yet
- Hfile: 49tcral Vsion-RDocument5 pagesHfile: 49tcral Vsion-RjannetolickaNo ratings yet
- NTSB Mab1919Document10 pagesNTSB Mab1919Kendric ShahidNo ratings yet
- Observation of Hurricane Impacts On Deepwater FacilitiesDocument15 pagesObservation of Hurricane Impacts On Deepwater FacilitiesMalik2202No ratings yet
- Narrative Report Module 11Document2 pagesNarrative Report Module 11Niña Edrienne JuntillaNo ratings yet
- Investigation into structural failure of cargo crane on Lodz 2Document27 pagesInvestigation into structural failure of cargo crane on Lodz 2TimmyJuri100% (1)
- National Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling ReportDocument5 pagesNational Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling ReportHELPPPPPNo ratings yet
- In Re: Governor'S Island Preservation and Education CorporationDocument20 pagesIn Re: Governor'S Island Preservation and Education CorporationCasey SeilerNo ratings yet
- Seacrest Drillship Sinking Investigation 1989Document128 pagesSeacrest Drillship Sinking Investigation 1989Divers Association100% (2)
- Q:/COMP/WATER2/OPA90: Oil Pollution Act of 1990Document66 pagesQ:/COMP/WATER2/OPA90: Oil Pollution Act of 1990Александр КохановскийNo ratings yet
- Sullivan Mine Fatalities Technical Investigations Summary ReportDocument20 pagesSullivan Mine Fatalities Technical Investigations Summary ReportEric GeorgeNo ratings yet
- OilSpillDisasterDocument23 pagesOilSpillDisasterAKASH KARANDENo ratings yet
- 524 2055 1 PB PDFDocument7 pages524 2055 1 PB PDFgalvigarciaNo ratings yet
- NR 1Document7 pagesNR 1pebita572No ratings yet
- ADVANCES IN UNDERWATER TECHNOLOGY OCEAN SCIENCE AND OFFSHORE ENGINEERING SubmersibleTechnology PDFDocument18 pagesADVANCES IN UNDERWATER TECHNOLOGY OCEAN SCIENCE AND OFFSHORE ENGINEERING SubmersibleTechnology PDFBuceo Mantto OCEAN INTREPIDNo ratings yet
- Accident Report - Cargo Gear FailureDocument19 pagesAccident Report - Cargo Gear FailureSanto IskandarNo ratings yet
- Operation Mount Hope III Documents From The ArmyDocument41 pagesOperation Mount Hope III Documents From The ArmyJohn GreenewaldNo ratings yet
- CREW: U.S. Coast Guard (USCG) : Regarding BP Oil Spill: 1/26/11 - FW NOC Phase 2 - Concern 0455-10 Update Report 44 - DEEPWATER HORIZONDocument10 pagesCREW: U.S. Coast Guard (USCG) : Regarding BP Oil Spill: 1/26/11 - FW NOC Phase 2 - Concern 0455-10 Update Report 44 - DEEPWATER HORIZONCREWNo ratings yet
- Marinecommunications1history AaronabbottstudentDocument4 pagesMarinecommunications1history Aaronabbottstudentapi-338525614No ratings yet
- Report of Operation Nanook PDFDocument111 pagesReport of Operation Nanook PDFFrankVarrecchioNo ratings yet
- M.S. Notice 1 of 1999Document1 pageM.S. Notice 1 of 1999Ajay SinghNo ratings yet
- Week2 - 211026 - CL7 - Lec - KojiGotohDocument9 pagesWeek2 - 211026 - CL7 - Lec - KojiGotohALT 000No ratings yet
- Satellite Application in Search and Rescue Operations: Presented by Group 4Document39 pagesSatellite Application in Search and Rescue Operations: Presented by Group 4basuNo ratings yet
- A Journey To 308 MetresDocument6 pagesA Journey To 308 MetresRon LoosNo ratings yet
- Catlin (Syndicate 2003) at Llo v. San Juan Towing & Marine Servi, 1st Cir. (2015)Document29 pagesCatlin (Syndicate 2003) at Llo v. San Juan Towing & Marine Servi, 1st Cir. (2015)Scribd Government DocsNo ratings yet
- Case Study - Human Factors AnalysisDocument14 pagesCase Study - Human Factors Analysismohamed ashorNo ratings yet
- Marinecommunications1history OishihawladerstudentDocument3 pagesMarinecommunications1history Oishihawladerstudentapi-331836063No ratings yet
- MS Notice 4 on HRU InstallationDocument1 pageMS Notice 4 on HRU Installationalive2flirtNo ratings yet
- Claude A DesgagnesDocument17 pagesClaude A DesgagnesEmanuel HuardNo ratings yet
- The Titan Submersible Implosion Was "An Accident Waiting To Happen" The New YorkerDocument35 pagesThe Titan Submersible Implosion Was "An Accident Waiting To Happen" The New YorkerFire DeerNo ratings yet
- Mai060823 FDocument19 pagesMai060823 FNayem PoshariNo ratings yet
- Star Sea insurance dispute over vessel seaworthiness and duty of disclosureDocument27 pagesStar Sea insurance dispute over vessel seaworthiness and duty of disclosureSyahirahNo ratings yet
- Structures Group Chairman's Factual ReportDocument7 pagesStructures Group Chairman's Factual ReportGFNo ratings yet
- Maritime: Edward Nonku Wanele Thingo Byron Andiswa WinstoneDocument11 pagesMaritime: Edward Nonku Wanele Thingo Byron Andiswa WinstonemahdouchfkiNo ratings yet
- Herald of Free Enterprise IntroDocument7 pagesHerald of Free Enterprise IntrothomasbranleyNo ratings yet
- FormalInvestigation HeraldofFreeEnterprise-MSA1894Document83 pagesFormalInvestigation HeraldofFreeEnterprise-MSA1894SU SHIPONNo ratings yet
- Itish EnterpriseDocument46 pagesItish EnterpriseCHEM PEACE100% (1)
- U. S. Naval Forces Vietnam Monthly Historical Summary Feb 1971Document116 pagesU. S. Naval Forces Vietnam Monthly Historical Summary Feb 1971Robert ValeNo ratings yet
- Bow Mariner Oil RecoveryDocument17 pagesBow Mariner Oil RecoverysasemarNo ratings yet
- Trouble With Steering Rudder Carrier: Return To TOCDocument2 pagesTrouble With Steering Rudder Carrier: Return To TOCRani NoumanNo ratings yet
- History of Offshore Oil and Gas in the United StatesDocument5 pagesHistory of Offshore Oil and Gas in the United StatesHELPPPPPNo ratings yet
- Geo Technical Investigation Volume 1Document23 pagesGeo Technical Investigation Volume 1Cele Adu-wusuNo ratings yet
- 2023-03-23-04-18-MCIB Black Magic ReportDocument64 pages2023-03-23-04-18-MCIB Black Magic ReportLionnel ParantNo ratings yet
- Marine Investigation Report M12L0147: TundraDocument26 pagesMarine Investigation Report M12L0147: TundraEmanuel HuardNo ratings yet
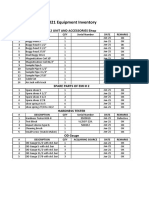
- 2021 Equipment Inventory: Emi 2 Unit and Accessories EitopDocument1 page2021 Equipment Inventory: Emi 2 Unit and Accessories Eitoptafani electricalNo ratings yet
- 2021 EMI Unit and Accessories InventoryDocument1 page2021 EMI Unit and Accessories Inventorytafani electricalNo ratings yet
- 2021 Equipment Inventory: Pin GrinderDocument1 page2021 Equipment Inventory: Pin Grindertafani electricalNo ratings yet
- Halliburton Interview QuestionsDocument8 pagesHalliburton Interview Questionspiolin8280% (5)
- IRI 750 Self-propelled Mechanical RigDocument1 pageIRI 750 Self-propelled Mechanical Rigtafani electricalNo ratings yet
- MacLean Electrical - IPG ManufacturersDocument2 pagesMacLean Electrical - IPG Manufacturerstafani electricalNo ratings yet
- Clinton Brian Selman NDT Quality Manager ResumeDocument2 pagesClinton Brian Selman NDT Quality Manager Resumetafani electricalNo ratings yet
- 2021 Equipment Inventory: Ultrasonic Flaw Detector & AccessoriesDocument1 page2021 Equipment Inventory: Ultrasonic Flaw Detector & Accessoriestafani electricalNo ratings yet
- IADC Specs Rig 12Document13 pagesIADC Specs Rig 12tafani electricalNo ratings yet
- 217966-Oil SpillDocument265 pages217966-Oil SpillAnonymous 4TfIMsDEJ8100% (1)
- History of The Offshore Oil & Gas Industry in Southern Louisiana - Vol 5Document1,266 pagesHistory of The Offshore Oil & Gas Industry in Southern Louisiana - Vol 5Faiz AhmadNo ratings yet
- Laminar and Turbulent FlowDocument305 pagesLaminar and Turbulent Flowjochem_ligthartNo ratings yet
- SIMOPS GuidelinesDocument13 pagesSIMOPS GuidelinesAmine Dabbabi100% (1)
- Shell - Oils - Deepwater - Mission - To - Mars (Ebook) PDFDocument108 pagesShell - Oils - Deepwater - Mission - To - Mars (Ebook) PDFantony grandeNo ratings yet
- Analysis of O & G Contract in GOMDocument208 pagesAnalysis of O & G Contract in GOMRuslan ZakirovNo ratings yet
- Deep Water Drilling TechnologyDocument896 pagesDeep Water Drilling TechnologyJesus Ponce GNo ratings yet
- Pete Slaiby Written StatementDocument4 pagesPete Slaiby Written StatementNational Commission on the BP Deepwater Horizon Oil Spill and Offshore DrillingNo ratings yet
- Republic of The Marshall Islands DEEPWATER HORIZON Marine Casualty Investigation Report-High ResolutionDocument216 pagesRepublic of The Marshall Islands DEEPWATER HORIZON Marine Casualty Investigation Report-High Resolutiondan_mcgraw73No ratings yet
- OCS Study Analyzes Instrument Performance for NC Oceanography ProgramDocument127 pagesOCS Study Analyzes Instrument Performance for NC Oceanography ProgramAniruddhNo ratings yet
- DecommissioningDocument280 pagesDecommissioningAnonymous ZO1piE3VNo ratings yet
- 2001 076Document152 pages2001 076YongJung KimNo ratings yet
- Fatigue Calculations for Existing Gulf of Mexico Fixed StructuresDocument115 pagesFatigue Calculations for Existing Gulf of Mexico Fixed StructuresImran Siddiqui100% (1)
- Benthos Long Branch USGSDocument45 pagesBenthos Long Branch USGSgrassle3482100% (3)
- Environmental Dredging ConsiderationsDocument441 pagesEnvironmental Dredging Considerationsvictoraboje100% (3)
- Notice: Native American Human Remains, Funerary Objects Inventory, Repatriation, Etc.: David Phelps Archaeology Laboratory of East Carolina University, Greenville, NCDocument3 pagesNotice: Native American Human Remains, Funerary Objects Inventory, Repatriation, Etc.: David Phelps Archaeology Laboratory of East Carolina University, Greenville, NCJustia.comNo ratings yet
- Offshore Oil Support Fact BookDocument148 pagesOffshore Oil Support Fact BookJuan Jose Alvarez Palma100% (1)
- In The United States Court of Appeals For The Fifth CircuitDocument6 pagesIn The United States Court of Appeals For The Fifth Circuiteditorial.onlineNo ratings yet
- Macondo Report 20042011Document33 pagesMacondo Report 20042011Dr K GallowglaichNo ratings yet
- Notice: Outer Continental Shelf Operations: Alaska Region— Beaufort Sea Oil and Gas Lease SalesDocument3 pagesNotice: Outer Continental Shelf Operations: Alaska Region— Beaufort Sea Oil and Gas Lease SalesJustia.comNo ratings yet
- Three Crane Accidents Caused by Improper RiggingDocument2 pagesThree Crane Accidents Caused by Improper RiggingSubbarao Mallampalli100% (1)
- Risk Management For Deepwater Oil DrillingDocument4 pagesRisk Management For Deepwater Oil Drillingvarunmunjal245No ratings yet
- Case16 - BP in The Gulf of MexicoDocument13 pagesCase16 - BP in The Gulf of MexicoZoo HuangNo ratings yet
- USCGSB Fixed Platform InspectionDocument40 pagesUSCGSB Fixed Platform Inspectionmarita2021No ratings yet
- 671AA-Final Report Offshore Electrical Cable Burial For Wind Farms PDFDocument220 pages671AA-Final Report Offshore Electrical Cable Burial For Wind Farms PDFnecmettinsengun50% (2)
- Api RP14Document4 pagesApi RP14Tudor virgilNo ratings yet
- DeepSpill Final ReportDocument159 pagesDeepSpill Final ReportJorge CiprianoNo ratings yet
- 3468Document161 pages3468Sir TemplarNo ratings yet
- Structure Equipment and Systems For Offshore Wind FarmsDocument252 pagesStructure Equipment and Systems For Offshore Wind Farmsfamiralis100% (4)
- Practical Reservoir Engineering and CharacterizationFrom EverandPractical Reservoir Engineering and CharacterizationRating: 4.5 out of 5 stars4.5/5 (3)
- Nuclear Energy in the 21st Century: World Nuclear University PressFrom EverandNuclear Energy in the 21st Century: World Nuclear University PressRating: 4.5 out of 5 stars4.5/5 (3)
- Renewable Energy: A Very Short IntroductionFrom EverandRenewable Energy: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (12)
- Power of Habit: The Ultimate Guide to Forming Positive Daily Habits, Learn How to Effectively Break Your Bad Habits For Good and Start Creating Good OnesFrom EverandPower of Habit: The Ultimate Guide to Forming Positive Daily Habits, Learn How to Effectively Break Your Bad Habits For Good and Start Creating Good OnesRating: 4.5 out of 5 stars4.5/5 (21)
- RV Living Collection: RV living for beginners, RV travel for the whole family, RV repair and RV mobile solar power: Experience Freedom on the roads alone or with your family with this collection. Learn how to repair your motorhome while using renewable energy!From EverandRV Living Collection: RV living for beginners, RV travel for the whole family, RV repair and RV mobile solar power: Experience Freedom on the roads alone or with your family with this collection. Learn how to repair your motorhome while using renewable energy!No ratings yet
- Biogas Production: Pretreatment Methods in Anaerobic DigestionFrom EverandBiogas Production: Pretreatment Methods in Anaerobic DigestionNo ratings yet
- Grid-Scale Energy Storage Systems and ApplicationsFrom EverandGrid-Scale Energy Storage Systems and ApplicationsFu-Bao WuNo ratings yet
- Offshore Wind Energy Generation: Control, Protection, and Integration to Electrical SystemsFrom EverandOffshore Wind Energy Generation: Control, Protection, and Integration to Electrical SystemsNo ratings yet
- Fundamentals of Hydrogen Production and Utilization in Fuel Cell SystemsFrom EverandFundamentals of Hydrogen Production and Utilization in Fuel Cell SystemsNo ratings yet
- Industrial Waste Treatment HandbookFrom EverandIndustrial Waste Treatment HandbookRating: 5 out of 5 stars5/5 (1)
- Global Landscape of Renewable Energy FinanceFrom EverandGlobal Landscape of Renewable Energy FinanceNo ratings yet
- Idaho Falls: The Untold Story of America's First Nuclear AccidentFrom EverandIdaho Falls: The Untold Story of America's First Nuclear AccidentRating: 4.5 out of 5 stars4.5/5 (21)
- Machine Learning and Data Science in the Oil and Gas Industry: Best Practices, Tools, and Case StudiesFrom EverandMachine Learning and Data Science in the Oil and Gas Industry: Best Practices, Tools, and Case StudiesPatrick BangertRating: 3 out of 5 stars3/5 (2)
- Shorting the Grid: The Hidden Fragility of Our Electric GridFrom EverandShorting the Grid: The Hidden Fragility of Our Electric GridRating: 4.5 out of 5 stars4.5/5 (2)
- The Boy Who Harnessed the Wind: Creating Currents of Electricity and HopeFrom EverandThe Boy Who Harnessed the Wind: Creating Currents of Electricity and HopeRating: 4 out of 5 stars4/5 (130)
- The Complete HVAC BIBLE for Beginners: The Most Practical & Updated Guide to Heating, Ventilation, and Air Conditioning Systems | Installation, Troubleshooting and Repair | Residential & CommercialFrom EverandThe Complete HVAC BIBLE for Beginners: The Most Practical & Updated Guide to Heating, Ventilation, and Air Conditioning Systems | Installation, Troubleshooting and Repair | Residential & CommercialNo ratings yet
- The New 3D Layout for Oil & Gas Offshore Projects: How to ensure successFrom EverandThe New 3D Layout for Oil & Gas Offshore Projects: How to ensure successRating: 4.5 out of 5 stars4.5/5 (3)
- ISO 50001: A strategic guide to establishing an energy management systemFrom EverandISO 50001: A strategic guide to establishing an energy management systemNo ratings yet
- The Way Home: Tales from a life without technologyFrom EverandThe Way Home: Tales from a life without technologyRating: 4 out of 5 stars4/5 (45)
- Power Quality in Power Systems and Electrical MachinesFrom EverandPower Quality in Power Systems and Electrical MachinesRating: 4.5 out of 5 stars4.5/5 (11)