You might also like
- Indonesia - Nursing Education Covid-19 PresentationDocument34 pagesIndonesia - Nursing Education Covid-19 PresentationUmu QonitunNo ratings yet
- A Handbook for Student Nurses, 2015–16 edition: Introducing Key Issues Relevant to PracticeFrom EverandA Handbook for Student Nurses, 2015–16 edition: Introducing Key Issues Relevant to PracticeRating: 5 out of 5 stars5/5 (2)
- Dossou 2018Document14 pagesDossou 2018Mensah AdolphNo ratings yet
- Bfci Hcws HandoutDocument68 pagesBfci Hcws HandoutBrianBeauttahNo ratings yet
- Quality and Outcomes Framework - What Have We Learnt?Document4 pagesQuality and Outcomes Framework - What Have We Learnt?Ana PaolaNo ratings yet
- Clinical Audit For Effective Delivery of Maternal Care in KenyaDocument41 pagesClinical Audit For Effective Delivery of Maternal Care in Kenyaskkrblsh100% (1)
- 2020 Practice - Implications - From - The - WCET - International.4Document8 pages2020 Practice - Implications - From - The - WCET - International.4durdane palabiyik yilmazNo ratings yet
- Introduction of TLD in South Africa Yogan PillayDocument14 pagesIntroduction of TLD in South Africa Yogan PillayBhekisisa HealthNo ratings yet
- RetrieveDocument2 pagesRetrieveJohn reinaNo ratings yet
- Jurnal Quality ImprovementDocument10 pagesJurnal Quality ImprovementbeungsyifaNo ratings yet
- Davao Regional Medical Center Public Health DepartmentDocument18 pagesDavao Regional Medical Center Public Health DepartmentGemma OrquioNo ratings yet
- Journal of Advanced Nursing - 2021 - Jacob - Pro Judge Study Nurses Professional Judgement in Nurse Staffing SystemsDocument8 pagesJournal of Advanced Nursing - 2021 - Jacob - Pro Judge Study Nurses Professional Judgement in Nurse Staffing SystemsenfaraujoNo ratings yet
- FIGO Postpartum Intrauterine Device Initiative: Complication Rates Across Six CountriesDocument8 pagesFIGO Postpartum Intrauterine Device Initiative: Complication Rates Across Six Countriesfarida yuni pertiwiNo ratings yet
- 7 PubmedDocument12 pages7 PubmedNydia Isabel Ruiz AntonioNo ratings yet
- Palliative Care Services Development FrameworkDocument64 pagesPalliative Care Services Development FrameworkHarun HarunovicNo ratings yet
- BJOG - 2023 - Category Abortion CareDocument3 pagesBJOG - 2023 - Category Abortion Care75dcqkm4nwNo ratings yet
- 16 Deeble Institute Issues Brief No. 16 Silk National Emergency Access Targets Aiming For The Target But What About The GoalDocument18 pages16 Deeble Institute Issues Brief No. 16 Silk National Emergency Access Targets Aiming For The Target But What About The Goaladhe irawanNo ratings yet
- CBFPDocument8 pagesCBFPadmasubregaNo ratings yet
- Translation of Evidence Into Nursing PracticeDocument8 pagesTranslation of Evidence Into Nursing PracticeNica C. MatsusakiNo ratings yet
- National Clinical Guideline No. 5 Clinical Handover Nov2014Document306 pagesNational Clinical Guideline No. 5 Clinical Handover Nov2014Ahmad JuliadiNo ratings yet
- Sepsis Management, National Clinical GuidelineNo. 6 (2020update) PDFDocument200 pagesSepsis Management, National Clinical GuidelineNo. 6 (2020update) PDFNg Khian LungNo ratings yet
- Pembicara - 1 - PROF FIONA ANMACDocument50 pagesPembicara - 1 - PROF FIONA ANMACTanaka IzzulhaqNo ratings yet
- Women and BirthDocument13 pagesWomen and BirthRobithoh AlamsyahNo ratings yet
- A Handbook for Student Nurses, 201617 edition: Introducing key issues relevant for practiceFrom EverandA Handbook for Student Nurses, 201617 edition: Introducing key issues relevant for practiceRating: 4 out of 5 stars4/5 (1)
- Department of Health - Women' S Health and Safe Motherhood Project - 2012-03-15Document8 pagesDepartment of Health - Women' S Health and Safe Motherhood Project - 2012-03-15daryl ann dep-asNo ratings yet
- Nanda-I, Noc, and Nic Linkages To Sars-Cov-2 (Covid-19) : Part 2. Individual ResponseDocument16 pagesNanda-I, Noc, and Nic Linkages To Sars-Cov-2 (Covid-19) : Part 2. Individual ResponseAprilia boddhiNo ratings yet
- Scaling Up Kangaroo Mother Care in The Philippines Using Policy, Regulatory and Systems Reform To Drive Changes in Birth PracticesDocument7 pagesScaling Up Kangaroo Mother Care in The Philippines Using Policy, Regulatory and Systems Reform To Drive Changes in Birth Practiceskaydee.arNo ratings yet
- Nursing Professional Governance Structure at Yale New Haven HospitalDocument4 pagesNursing Professional Governance Structure at Yale New Haven HospitalNurulfitrahhafidNo ratings yet
- Columbia-Presbyterian Patient Safety StudyDocument9 pagesColumbia-Presbyterian Patient Safety StudyKathleen Beatty100% (1)
- Chesterfield MDT ReviewDocument20 pagesChesterfield MDT ReviewLinda WalkerNo ratings yet
- A Handbook for Student Nurses, 201819 edition: Introducing key issues relevant for practiceFrom EverandA Handbook for Student Nurses, 201819 edition: Introducing key issues relevant for practiceNo ratings yet
- Adolescent Girls' Nutrition and Prevention of Anaemia: A School Based Multisectoral Collaboration in IndonesiaDocument6 pagesAdolescent Girls' Nutrition and Prevention of Anaemia: A School Based Multisectoral Collaboration in IndonesiamamaazkaNo ratings yet
- Ewsletter: National Newborn Health ProgramDocument8 pagesEwsletter: National Newborn Health ProgramFarjana JahanNo ratings yet
- International Guidelines For The Management of Septic Shock & Sepsis-Associated Organ Dysfunction in Children (SSCGC)Document97 pagesInternational Guidelines For The Management of Septic Shock & Sepsis-Associated Organ Dysfunction in Children (SSCGC)EstebanNo ratings yet
- Standard For Hospital Providing Neonatal Intensibe Care and High Dependency CareDocument22 pagesStandard For Hospital Providing Neonatal Intensibe Care and High Dependency CareDouglas MenjivarNo ratings yet
- Trend Analysis of The Nursing Shortage in CanadaDocument11 pagesTrend Analysis of The Nursing Shortage in Canadaelliott.allmanNo ratings yet
- Recall Intervals and NICE GuidelinesDocument7 pagesRecall Intervals and NICE Guidelinesdruzair007No ratings yet
- Quality Issu in Midwifery ICM PDFDocument9 pagesQuality Issu in Midwifery ICM PDFFarhatiNo ratings yet
- National Contraception Clinical GuidelinesDocument110 pagesNational Contraception Clinical GuidelinesPrecious NkadimengNo ratings yet
- Kidney Careoutline1203Document3 pagesKidney Careoutline1203weesiniNo ratings yet
- A Second Set of Eyes An Introduction To Tele-ICUDocument12 pagesA Second Set of Eyes An Introduction To Tele-ICUvijju006No ratings yet
- SCC South AfricaDocument13 pagesSCC South AfricaVictoria SalazarNo ratings yet
- Nursing Informatics (Lecture) Chapter Summary: Ateneo de Naga University College of Nursing 4400, Naga City, PhilippinesDocument10 pagesNursing Informatics (Lecture) Chapter Summary: Ateneo de Naga University College of Nursing 4400, Naga City, PhilippinesGabrielle EvangelistaNo ratings yet
- Fetal Monitoring in Labour: Summary and Update of NICE GuidanceDocument4 pagesFetal Monitoring in Labour: Summary and Update of NICE GuidanceMitsury Jacqueline Flores C.No ratings yet
- College Statement: Policy Statement On Shared Maternity Care Obstetric Patients in Australia WPI-9Document4 pagesCollege Statement: Policy Statement On Shared Maternity Care Obstetric Patients in Australia WPI-9Ywagar YwagarNo ratings yet
- India Situation Report 73Document3 pagesIndia Situation Report 73dhivyascrNo ratings yet
- Future of NursingDocument6 pagesFuture of Nursingsnave kibetNo ratings yet
- Consensus on Best Practices for IUC in FranceDocument10 pagesConsensus on Best Practices for IUC in FranceJuly López LeitonNo ratings yet
- PD2019_020Document11 pagesPD2019_020hatem newishyNo ratings yet
- Building An NCD-ready Workforce: Technical Meeting ReportDocument48 pagesBuilding An NCD-ready Workforce: Technical Meeting ReportnavenNo ratings yet
- WHO STAGE Advisory Group Discusses Mitigating COVID-19 Impacts on MNCAHNDocument33 pagesWHO STAGE Advisory Group Discusses Mitigating COVID-19 Impacts on MNCAHNAbebe TilahunNo ratings yet
- Journal of Clinical Nursing - 2021 - Arsenault Knudsen - The Realities of Practice Change Nurses PerceptionsDocument12 pagesJournal of Clinical Nursing - 2021 - Arsenault Knudsen - The Realities of Practice Change Nurses Perceptionsxisici5890No ratings yet
- ICM Global Standards for Midwifery EducationDocument11 pagesICM Global Standards for Midwifery EducationMumtihana MuchlisNo ratings yet
- Jurnal 1Document12 pagesJurnal 1Riafinola IfanisariNo ratings yet
- Responsiveness of Health Systems To Patient Needs: 12. Serving CitizensDocument3 pagesResponsiveness of Health Systems To Patient Needs: 12. Serving CitizensWulan PurwantyNo ratings yet
- DoH Preceptorship AHPs, Nurses MidwiferyDocument33 pagesDoH Preceptorship AHPs, Nurses MidwiferyAnisah Tifani MaulidyantiNo ratings yet
- 2012rh CommunitymidwiferyguidelinesDocument43 pages2012rh Communitymidwiferyguidelinesgeorgeloto12100% (1)
- The Impact of National Health Ensurance Scheme On Enrollees in Gombe Metropolis, Gombe State NigeriaDocument10 pagesThe Impact of National Health Ensurance Scheme On Enrollees in Gombe Metropolis, Gombe State NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blueprint Transition Report - 2015 - ENGDocument8 pagesBlueprint Transition Report - 2015 - ENGcopataganNo ratings yet
- Nur 436 Psi 17 PresentationDocument21 pagesNur 436 Psi 17 Presentationapi-689882394No ratings yet
- Trade Unionists and EnvironmentalismDocument18 pagesTrade Unionists and EnvironmentalismGrant BrookesNo ratings yet
- President's Information To Board and MembersDocument51 pagesPresident's Information To Board and MembersGrant BrookesNo ratings yet
- Policy Remit 2 - Full Independent Review of The NZNO ConstitutionDocument1 pagePolicy Remit 2 - Full Independent Review of The NZNO ConstitutionGrant BrookesNo ratings yet
- Review of The New Zealand Nurses Organisation District Health Board MECA Bargaining and Campaign Process 2017-18Document87 pagesReview of The New Zealand Nurses Organisation District Health Board MECA Bargaining and Campaign Process 2017-18Grant BrookesNo ratings yet
- C489 Task1 CompletedDocument4 pagesC489 Task1 CompletedSteven SteveNo ratings yet
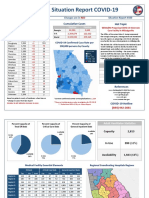
- 6-24-20 - Georgia Situation Report COVIDDocument2 pages6-24-20 - Georgia Situation Report COVIDWCTV Digital TeamNo ratings yet
- Bozeman Deaconess Proposal For Big Sky HospitalDocument48 pagesBozeman Deaconess Proposal For Big Sky HospitalBozeman Daily ChronicleNo ratings yet
- Intrapreneurship at DaVita Health Care PartnersDocument4 pagesIntrapreneurship at DaVita Health Care PartnersHaseeb AhmedNo ratings yet
- Hospital Marketing StrategyDocument15 pagesHospital Marketing StrategyKomal SaneNo ratings yet
- Rayat HospitalDocument1 pageRayat HospitalSiddhesh ShahNo ratings yet
- (Honduras) : Mental Health ATLAS 2020 - Member State ProfileDocument3 pages(Honduras) : Mental Health ATLAS 2020 - Member State ProfileJosé Pablo Funes SánchezNo ratings yet
- Strategic Management - 2 AssignmentDocument11 pagesStrategic Management - 2 Assignmentpushkar morankarNo ratings yet
- Business Plan - Retail Hospital PharmacyDocument14 pagesBusiness Plan - Retail Hospital PharmacyVNcomer100% (10)
- Two-Way Referral Form PDFDocument1 pageTwo-Way Referral Form PDFcatherine joy macalos100% (4)
- Proper home visit proceduresDocument2 pagesProper home visit procedureslea mae andoloyNo ratings yet
- Session #10 SAS - TFNDocument10 pagesSession #10 SAS - TFNKristina CassandraNo ratings yet
- APNs: Access, Cost, Quality Care & EnvironmentsDocument6 pagesAPNs: Access, Cost, Quality Care & EnvironmentsMellyne SallyNo ratings yet
- Nursing Implications Filipino & German HeritageDocument4 pagesNursing Implications Filipino & German HeritageArmstrong AsenaviNo ratings yet
- 6.bartels (1987)Document9 pages6.bartels (1987)Pablo Ferrer GonzalezNo ratings yet
- Journal Medical WardDocument5 pagesJournal Medical WardDarren FloresNo ratings yet
- 111 HospitalsDocument1 page111 HospitalsNatalie EvansNo ratings yet
- Prevalence of and Factors Associated With Nurse Burnout in The USDocument11 pagesPrevalence of and Factors Associated With Nurse Burnout in The USSMA N 1 TOROHNo ratings yet
- Detoxification and Substance Abuse Treatment TIP 45 U.S.Document269 pagesDetoxification and Substance Abuse Treatment TIP 45 U.S.mmoslem100% (2)
- Determinants of Parental Decisions On 'Drop Out' From Cancer Treatment For Childhood Cancer PatientsDocument7 pagesDeterminants of Parental Decisions On 'Drop Out' From Cancer Treatment For Childhood Cancer PatientsAndrew HartonoNo ratings yet
- Patient and Management Perspectives on Emergency Room QualityDocument10 pagesPatient and Management Perspectives on Emergency Room QualityBenn TennNo ratings yet
- Weeks 11 - Pair A&BDocument4 pagesWeeks 11 - Pair A&BSuryakant KaushikNo ratings yet
- Cancer Bathinda's Dubious DistinctionDocument2 pagesCancer Bathinda's Dubious DistinctionPardeepSinghNo ratings yet
- Drop ReqDocument20 pagesDrop Reqwace marikuzaNo ratings yet
- RPN Priority and Delegation Practice Test QuestionsDocument5 pagesRPN Priority and Delegation Practice Test Questionsfairwoods0% (2)
- The Nurse Manager's Guide To Innovative Staffing - IntroductionDocument6 pagesThe Nurse Manager's Guide To Innovative Staffing - IntroductionBrent PatrickNo ratings yet
- PhilHealth Hospital Accreditation ChecklistDocument14 pagesPhilHealth Hospital Accreditation Checklistamira_hassan100% (1)
- CGASDocument4 pagesCGASDinny Atin AmanahNo ratings yet
- A Prospective Treatment Protocol For Outpatient Laparoscopic Appendectomy For Acute AppendicitisDocument5 pagesA Prospective Treatment Protocol For Outpatient Laparoscopic Appendectomy For Acute AppendicitisBenjamin PaulinNo ratings yet
- Clinical Guideline: Management of Patients With Vancomycin-Resistant Enterococci (VRE) Clinical GuidelineDocument25 pagesClinical Guideline: Management of Patients With Vancomycin-Resistant Enterococci (VRE) Clinical GuidelinedanielaNo ratings yet