You might also like
- Applied Mathematics 10 (Zambak) - Zambak Publishing (2008) PDFDocument200 pagesApplied Mathematics 10 (Zambak) - Zambak Publishing (2008) PDFdata100% (1)
- I Recognize That My Freshman ExperienceDocument6 pagesI Recognize That My Freshman ExperienceWander LustNo ratings yet
- LimbDocument15 pagesLimbGiorgio AgazziNo ratings yet
- Cegielski2021 Article CombinedInVivoMuscleMassMuscleDocument13 pagesCegielski2021 Article CombinedInVivoMuscleMassMuscleErick Mosquera LópezNo ratings yet
- TensDocument9 pagesTensRiri NandaNo ratings yet
- Skeletal Muscle Protein Synthesis and mTORC1 Nutritional and Contractile Regulation of HumanDocument12 pagesSkeletal Muscle Protein Synthesis and mTORC1 Nutritional and Contractile Regulation of HumankalikNo ratings yet
- JMD 19083Document3 pagesJMD 19083anton MDNo ratings yet
- Dosagem Otima Musculo PDFDocument10 pagesDosagem Otima Musculo PDFJanaina PanizzaNo ratings yet
- Whey Protein But Not Collagen Peptides Stimulate Acute and Longer Term Muscle Protein SynthesisDocument11 pagesWhey Protein But Not Collagen Peptides Stimulate Acute and Longer Term Muscle Protein SynthesisFlávia Sobreira NutricionistaNo ratings yet
- Wavelet Analysis of Rearfoot Loading of Patients After Medial Patellofemoral Ligament MPFL ReconstructionDocument6 pagesWavelet Analysis of Rearfoot Loading of Patients After Medial Patellofemoral Ligament MPFL ReconstructionceydaalyazhotamisNo ratings yet
- Expresi PeriostinDocument5 pagesExpresi Periostinkhoirul imaNo ratings yet
- Kiper2015 Propio PDFDocument6 pagesKiper2015 Propio PDFJuan Pedro BarrientosNo ratings yet
- Smudging of The Motor Cortex Is Related To The Severity of Low Back PainDocument18 pagesSmudging of The Motor Cortex Is Related To The Severity of Low Back PainAugusto Felipe Benavides MejiasNo ratings yet
- Accepted Manuscript: 10.1016/j.apmr.2016.08.481Document14 pagesAccepted Manuscript: 10.1016/j.apmr.2016.08.481Vivin YulvinaNo ratings yet
- Vastus Medialis PDFDocument5 pagesVastus Medialis PDFdespNo ratings yet
- Moghadam2020 Article TheEffectsOfConcurrentTrainingDocument9 pagesMoghadam2020 Article TheEffectsOfConcurrentTrainingamirreza jmNo ratings yet
- The Effects of Poliomyelitis On Motor Unit Behavior During Repetitive Muscle Actions: A Case ReportDocument7 pagesThe Effects of Poliomyelitis On Motor Unit Behavior During Repetitive Muscle Actions: A Case ReportUswatun HasanahNo ratings yet
- Whey Protein But Not Collagen Peptides Stimulate Acute and Longer-Term Muscle Protein Synthesis With and Without Resistance Exercise in Healthy Older Women: A Randomized Controlled TrialDocument11 pagesWhey Protein But Not Collagen Peptides Stimulate Acute and Longer-Term Muscle Protein Synthesis With and Without Resistance Exercise in Healthy Older Women: A Randomized Controlled TrialElson TavaresNo ratings yet
- BiomekanikDocument2 pagesBiomekanikBrinna Anindita SatriaNo ratings yet
- Effects of Creatine Supplementation On The Energy Cost of Muscle ContractionDocument9 pagesEffects of Creatine Supplementation On The Energy Cost of Muscle ContractionCharisNo ratings yet
- Exercise and Regulation of Protein MetabolismDocument24 pagesExercise and Regulation of Protein MetabolismTheofilus ArdyNo ratings yet
- Architectural, Functional and Molecular Responses To Concentric and Eccentric Loading in Human Skeletal MuscleDocument14 pagesArchitectural, Functional and Molecular Responses To Concentric and Eccentric Loading in Human Skeletal MuscleSheilani MartinsNo ratings yet
- Variabilidade Da Arquitetura Regional Do Quadríceps em Homens Treinados Avaliados Pelo Modo B e Ultrassonografia de Campo de Visão EstendidoDocument17 pagesVariabilidade Da Arquitetura Regional Do Quadríceps em Homens Treinados Avaliados Pelo Modo B e Ultrassonografia de Campo de Visão Estendidoleal thiagoNo ratings yet
- Sensorimotor Control Deficiency in Recurrent Anterior Shoulder Instability Assessed With A Stabilometric Force PlatformDocument6 pagesSensorimotor Control Deficiency in Recurrent Anterior Shoulder Instability Assessed With A Stabilometric Force PlatformA ANo ratings yet
- 2009 Kapreli Anterior Cruciate Ligament Deficiency Causes Brain Plasticity A Functional MRI StudyDocument8 pages2009 Kapreli Anterior Cruciate Ligament Deficiency Causes Brain Plasticity A Functional MRI StudyArmin ParavlićNo ratings yet
- Lower Extremity Muscle Activation During Functional Exercises in Patients With and Without Chronic Ankle InstabilityDocument10 pagesLower Extremity Muscle Activation During Functional Exercises in Patients With and Without Chronic Ankle InstabilityDavid SugiartoNo ratings yet
- I P P I I R E P: Schemic Reconditioning and Lacebo Ntervention Mproves Esistance Xercise ErformanceDocument8 pagesI P P I I R E P: Schemic Reconditioning and Lacebo Ntervention Mproves Esistance Xercise ErformanceBatta ZahranNo ratings yet
- D'Oliveira - Physical Exercise Is Associated With Better Fat Mass Distribution and Lower Insulin Resistance in Spinal Cord Injured IndividualsDocument6 pagesD'Oliveira - Physical Exercise Is Associated With Better Fat Mass Distribution and Lower Insulin Resistance in Spinal Cord Injured Individuals2fns74m6fnNo ratings yet
- A Single-Blind, Cross-Over Trial of Hip Abductor Strength Training To Improve Timed Up Go Performance in Patients With Unilateral, Transfemoral AmputationDocument7 pagesA Single-Blind, Cross-Over Trial of Hip Abductor Strength Training To Improve Timed Up Go Performance in Patients With Unilateral, Transfemoral AmputationJhony GonzalezNo ratings yet
- A Randomized Controlled Trial of Angiotensin-Converting Enzyme Inhibition For Skeletal Muscle Dysfunction in COPDDocument9 pagesA Randomized Controlled Trial of Angiotensin-Converting Enzyme Inhibition For Skeletal Muscle Dysfunction in COPDᄋᄋNo ratings yet
- Effects of Continuous Passive Motion On Reversing The Adapted Spinal Circuit in Humans With Chronic Spinal Cord InjuryDocument7 pagesEffects of Continuous Passive Motion On Reversing The Adapted Spinal Circuit in Humans With Chronic Spinal Cord InjuryJoy SantosNo ratings yet
- 51 FullDocument8 pages51 FullsillNo ratings yet
- Populasi 18Document8 pagesPopulasi 18Resky Ika Sah PutriNo ratings yet
- Changes in Calf Muscle Elasticity in Hypogonadal Males Before and After Testosterone Substitution As Monitored by Magnetic Resonance ElastographyDocument6 pagesChanges in Calf Muscle Elasticity in Hypogonadal Males Before and After Testosterone Substitution As Monitored by Magnetic Resonance ElastographyKevin BimarigaNo ratings yet
- Appes Abstracts: Oral PresentationsDocument146 pagesAppes Abstracts: Oral PresentationsstoneNo ratings yet
- Accepted Manuscript: 10.1016/j.jbmt.2016.06.011Document20 pagesAccepted Manuscript: 10.1016/j.jbmt.2016.06.011Daniel GuevaraNo ratings yet
- 1 s2.0 S1388245719310041 MainDocument1 page1 s2.0 S1388245719310041 MainMohamed AbdoNo ratings yet
- Abnormal Mitochondrial Function and Muscle Wasting, But Normal Contractile Efficiency, in Haemodialysed Patients Studied Non-Invasively in VivoDocument8 pagesAbnormal Mitochondrial Function and Muscle Wasting, But Normal Contractile Efficiency, in Haemodialysed Patients Studied Non-Invasively in VivoDaniel Fernando Mendez CarbajalNo ratings yet
- T 202200883Document7 pagesT 202200883i'm KaiyNo ratings yet
- Robotic Arm-Assisted Versus Manual Total Hip Arthroplasty A Propensity Score Matched Cohort StudyDocument9 pagesRobotic Arm-Assisted Versus Manual Total Hip Arthroplasty A Propensity Score Matched Cohort StudyShiv KolheNo ratings yet
- Resistance Exercise-Induced Regulation of Muscle Protein Synthesis To Intraset RestDocument35 pagesResistance Exercise-Induced Regulation of Muscle Protein Synthesis To Intraset RestMacarena Beatriz Artigas AriasNo ratings yet
- Force-Controlled Biting Alters Postural Control in BipedalDocument13 pagesForce-Controlled Biting Alters Postural Control in BipedalSamNo ratings yet
- ArticleDocument11 pagesArticleSai RamNo ratings yet
- Electromyographic Analysis of Pelvic Floor Muscles During The Execution of Pelvic Patterns of Proprioceptive Neuromuscular Facilitation ConceptDocument10 pagesElectromyographic Analysis of Pelvic Floor Muscles During The Execution of Pelvic Patterns of Proprioceptive Neuromuscular Facilitation Conceptg7ccbb2pw9No ratings yet
- Improved 4-Compartment Body-Composition Model For A Clinically Accessible Measure of Total Body ProteinDocument8 pagesImproved 4-Compartment Body-Composition Model For A Clinically Accessible Measure of Total Body ProteinVaneariasNo ratings yet
- EMG en UCI - Club de Revista PDFDocument6 pagesEMG en UCI - Club de Revista PDFJOSE JULIAN BERNAL SANCHEZNo ratings yet
- BackgroundDocument15 pagesBackgroundcony.juulNo ratings yet
- Bio Marcadores en Sarcopenia Calvani2017Document6 pagesBio Marcadores en Sarcopenia Calvani2017JAVIER VELASQUEZ100% (1)
- Leveraging Subject-Specific Musculoskeletal Modeling To Assess Effect of Anterior Cruciate Ligament Retaining Total Knee Arthroplasty During Walking GaitDocument12 pagesLeveraging Subject-Specific Musculoskeletal Modeling To Assess Effect of Anterior Cruciate Ligament Retaining Total Knee Arthroplasty During Walking GaitWami FadelNo ratings yet
- The Rolf Method of Structural IntegratioDocument13 pagesThe Rolf Method of Structural IntegratioTaune AntonioNo ratings yet
- AclDocument10 pagesAclckpravin7754No ratings yet
- 2307 FullDocument8 pages2307 FulldruidsamsungNo ratings yet
- 410 4225 PDFDocument5 pages410 4225 PDFmilhimNo ratings yet
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- Avaliação QuadrilDocument27 pagesAvaliação QuadrilMarcus Dos SantosNo ratings yet
- Beats-A Accessibility 3D Imprinted Unit Pertaining To in Vitro Electromechanical Excitement Regarding Human Activated Pluripotent Come TissueDocument2 pagesBeats-A Accessibility 3D Imprinted Unit Pertaining To in Vitro Electromechanical Excitement Regarding Human Activated Pluripotent Come Tissueelbowcable7No ratings yet
- 2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseDocument23 pages2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseFrancisco Antonó Castro WeithNo ratings yet
- Nuclear Magnetic Phosphates And: 31P Resonance Studies of PH in Human MuscleDocument7 pagesNuclear Magnetic Phosphates And: 31P Resonance Studies of PH in Human MuscleRoque Esteban Beltran GallardoNo ratings yet
- Sarcopenia TacDocument5 pagesSarcopenia TacIvan ChavezNo ratings yet
- Correlation Between Maximal Inspiratory Pressure With Six Minutes Walking Test and Copd Assessment Test ScoreDocument1 pageCorrelation Between Maximal Inspiratory Pressure With Six Minutes Walking Test and Copd Assessment Test ScorerifkymubarakNo ratings yet
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 3: Heart, Lymph Node and Musculoskeletal System: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTFrom EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 3: Heart, Lymph Node and Musculoskeletal System: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNo ratings yet
- 131I Therapy For Elevated Thyroglobulin LevelsDocument8 pages131I Therapy For Elevated Thyroglobulin LevelsMeutia sariNo ratings yet
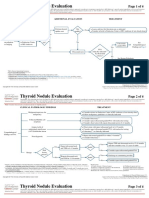
- Clin Management Thyroid Nodule Eval Web AlgorithmDocument4 pagesClin Management Thyroid Nodule Eval Web AlgorithmMeutia sariNo ratings yet
- (TC) - 99m Thyroid Scintigraphy in Congenital Hypothyroidism Screening ProgramDocument5 pages(TC) - 99m Thyroid Scintigraphy in Congenital Hypothyroidism Screening ProgramMeutia sariNo ratings yet
- Congenital Hypothyroidism Follow Up of A Case For 13 Years PDFDocument14 pagesCongenital Hypothyroidism Follow Up of A Case For 13 Years PDFMeutia sariNo ratings yet
- Kebijakan Penggunaan ApronDocument61 pagesKebijakan Penggunaan ApronMeutia sariNo ratings yet
- Permenkes Tentang Penetapan Nilai KritisDocument34 pagesPermenkes Tentang Penetapan Nilai KritisMeutia sariNo ratings yet
- Kebijakan Pelayanan RadiologiDocument32 pagesKebijakan Pelayanan RadiologiMeutia sariNo ratings yet
- 5Document10 pages5Meutia sariNo ratings yet
- 2021-09-Network Design and Troubleshooting Assign-PART1Document10 pages2021-09-Network Design and Troubleshooting Assign-PART1Firdous JamalNo ratings yet
- Avoiding Shifts in Person, Number and TenseDocument3 pagesAvoiding Shifts in Person, Number and Tenseteachergrace1225No ratings yet
- History of OperaDocument8 pagesHistory of OperaNachoAndrésLlorenteNo ratings yet
- The Wanderer & Seafearer - 230228 - 151524Document8 pagesThe Wanderer & Seafearer - 230228 - 151524Nikolett LakatosNo ratings yet
- Tle 10 Week 1-4 Las 1 and 2Document2 pagesTle 10 Week 1-4 Las 1 and 2I See Tech BasicNo ratings yet
- Universidad Autonoma de Chiriqui Extension de Boquete Pmi 700 Language AcquisitionDocument8 pagesUniversidad Autonoma de Chiriqui Extension de Boquete Pmi 700 Language AcquisitionGénesis Liriola Morales VillarrealNo ratings yet
- Rejda rmiGE ppt01Document25 pagesRejda rmiGE ppt01Fadi OsamaNo ratings yet
- Introduction To LauncherDocument9 pagesIntroduction To LauncherNathalia0% (1)
- How Project Leaders Can Overcome The Crisis of SilenceDocument12 pagesHow Project Leaders Can Overcome The Crisis of SilenceKrunal DattaniNo ratings yet
- Format Incident Report New 2019Document2 pagesFormat Incident Report New 2019Meliza RollanNo ratings yet
- DifferentiationsDocument20 pagesDifferentiationsShreyansh KashaudhanNo ratings yet
- Feasibility Study (Compatibility Mode)Document35 pagesFeasibility Study (Compatibility Mode)Deep ShahNo ratings yet
- Az-900 PrepAway PDFDocument82 pagesAz-900 PrepAway PDFNisha PrasadNo ratings yet
- Writing A Review - Guidelines and WorksheetDocument9 pagesWriting A Review - Guidelines and WorksheetBaz MonstruosoNo ratings yet
- A Letter To A Friend - Ela-Writing Lesson PlanDocument5 pagesA Letter To A Friend - Ela-Writing Lesson Planapi-642378584No ratings yet
- 2023-2024 Binhi Letter To ParentsDocument2 pages2023-2024 Binhi Letter To ParentsMiggy AquinoNo ratings yet
- Marketing Research Report:Netflix: Presented By: Rida Ahmad Ali Jawad Meeral ZiaDocument12 pagesMarketing Research Report:Netflix: Presented By: Rida Ahmad Ali Jawad Meeral ZiaAli JawadNo ratings yet
- AIDS Is Man-Made by William CooperDocument3 pagesAIDS Is Man-Made by William CooperPeter100% (3)
- Online Voting SystemDocument20 pagesOnline Voting SystemArihant PawariyaNo ratings yet
- Bus 5115 - Discussion Forum Unit 1 University of The PeopleDocument5 pagesBus 5115 - Discussion Forum Unit 1 University of The Peoplechristian allosNo ratings yet
- Ihcdc 2021Document2 pagesIhcdc 2021Wisnu WiwekaNo ratings yet
- Xen'drik Expedition To Tomb of AnnihilationDocument7 pagesXen'drik Expedition To Tomb of AnnihilationkalicjawaczykNo ratings yet
- Agbay V Deputy OmbudsmanDocument2 pagesAgbay V Deputy Ombudsmannina100% (5)
- Britni Freiboth's Resume 2010Document2 pagesBritni Freiboth's Resume 2010api-51238443No ratings yet
- SocialDocument4 pagesSocialPankaj ChetryNo ratings yet
- TS BRANDING ResearchDocument11 pagesTS BRANDING ResearchPARITOSH SHARMANo ratings yet
- FAQs in C LanguageDocument256 pagesFAQs in C LanguageShrinivas A B0% (2)
- Jan Scholten Repertory of The Elements 5994eceb1723ddd169543dffDocument3 pagesJan Scholten Repertory of The Elements 5994eceb1723ddd169543dffUsman AnsariNo ratings yet