You might also like
- Fast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaFrom EverandFast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaNo ratings yet
- Vital-Sign Abnormalities As Predictors of Pneumonia in Adults With Acute Cough IllnessDocument6 pagesVital-Sign Abnormalities As Predictors of Pneumonia in Adults With Acute Cough IllnessMazKha BudNo ratings yet
- Covid 19 Guidelines April 2021Document42 pagesCovid 19 Guidelines April 2021K.sushmaNo ratings yet
- Interpretation of Tests for Diagnosing Rheumatic FeverDocument3 pagesInterpretation of Tests for Diagnosing Rheumatic FeverAl- Mondjid LeeNo ratings yet
- 5754-Article Text-43741-3-10-20220520Document18 pages5754-Article Text-43741-3-10-20220520Ricardo TanNo ratings yet
- Challenges in The Diagnosis of Wilson Disease: Aurélia Poujois, France WoimantDocument10 pagesChallenges in The Diagnosis of Wilson Disease: Aurélia Poujois, France WoimantHadi KuriryNo ratings yet
- Gout and The Risk of Epilepsy A Population Based.44Document6 pagesGout and The Risk of Epilepsy A Population Based.44Afni Panggar BesiNo ratings yet
- A 19 Year Old With Fever, Rash, and Conjunctivitis: A Connection With The HeartDocument3 pagesA 19 Year Old With Fever, Rash, and Conjunctivitis: A Connection With The HeartLeberina TunjNo ratings yet
- Guide For Diagnosis of ARFDocument2 pagesGuide For Diagnosis of ARFpatyoungNo ratings yet
- Acute Rheumatic Fever: Cme R ADocument5 pagesAcute Rheumatic Fever: Cme R ABinod KumarNo ratings yet
- Brainsci 13 00450Document7 pagesBrainsci 13 00450Krit KritNo ratings yet
- 2022 ITECritiqueDocument80 pages2022 ITECritiqueJon LetkoNo ratings yet
- Chapter 2Document14 pagesChapter 2rahayusri yayuNo ratings yet
- Sepsis 2Document14 pagesSepsis 2ROCIO Vasquez OVALLENo ratings yet
- International Journal of Scientific Research: General MedicineDocument4 pagesInternational Journal of Scientific Research: General MedicineTriple ANo ratings yet
- Full Guidelines ManuscriptDocument44 pagesFull Guidelines ManuscriptDesak PramestiNo ratings yet
- Jones Criteria and Underdiagnosis of Rheumatic FeverDocument6 pagesJones Criteria and Underdiagnosis of Rheumatic FeverVanitha Ratha KrishnanNo ratings yet
- Clinical Patterns of Kawasaki Disease and Factors Associated With Echocardiography Abnormalities at Presentation Libyan ExperienceDocument7 pagesClinical Patterns of Kawasaki Disease and Factors Associated With Echocardiography Abnormalities at Presentation Libyan ExperienceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Research Paper On LupusDocument4 pagesResearch Paper On Lupusfyrj7h9z100% (1)
- Predicting Benign Course and Prolonged Illness in Lower Respiratory Tract Infections: A 13 European Country StudyDocument8 pagesPredicting Benign Course and Prolonged Illness in Lower Respiratory Tract Infections: A 13 European Country Studypanji satryo utomoNo ratings yet
- 1476 1645 Article p479Document6 pages1476 1645 Article p479Yuyun RasulongNo ratings yet
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDocument5 pagesCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarNo ratings yet
- Sepsis in Older PatientsDocument8 pagesSepsis in Older PatientsFajar WasilahNo ratings yet
- Characteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterDocument9 pagesCharacteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterFrancescFranquesaNo ratings yet
- AAFP SepsisDocument13 pagesAAFP SepsisANISA RACHMITA ARIANTI 2020No ratings yet
- 35-Article Text-212-1-10-20200524Document4 pages35-Article Text-212-1-10-20200524SONIA AGUILAR RIVERANo ratings yet
- Urinary/Kidney Disorders - Health Policy & RegulatoryDocument1 pageUrinary/Kidney Disorders - Health Policy & RegulatoryYehezkiel Nathanael SiahaanNo ratings yet
- Rheumatic Heart Disease in Developing Countries: PerspectiveDocument3 pagesRheumatic Heart Disease in Developing Countries: PerspectiveStephannia OidorNo ratings yet
- Role of Alvarado Score in The Diagnosis of Acute AppendicitisDocument5 pagesRole of Alvarado Score in The Diagnosis of Acute AppendicitisMahlina Nur LailiNo ratings yet
- 93 1373875972 PDFDocument5 pages93 1373875972 PDFMahlina Nur LailiNo ratings yet
- Criteri 205 Johnes PDFDocument7 pagesCriteri 205 Johnes PDFTeodor ŞişianuNo ratings yet
- Literature Review of Rheumatic Heart DiseaseDocument5 pagesLiterature Review of Rheumatic Heart Diseaseafdtakoea100% (1)
- Connective Tissue Disease-Associated Interstitial Lung Diseases: Unresolved IssuesDocument9 pagesConnective Tissue Disease-Associated Interstitial Lung Diseases: Unresolved IssuesNuntana ChampaNo ratings yet
- Term Paper Rheumatic FeverDocument6 pagesTerm Paper Rheumatic Fevereubvhsvkg100% (1)
- Lepto SpirosDocument8 pagesLepto SpirosNisa UcilNo ratings yet
- Acute Hepatitis Technical Briefing 2Document49 pagesAcute Hepatitis Technical Briefing 2diahsenoNo ratings yet
- Acute Rheumatic Fever Clinical Profile in Children in Western UkraineDocument5 pagesAcute Rheumatic Fever Clinical Profile in Children in Western UkraineraniaulfahNo ratings yet
- Plante-2016-Management of Sepsis and Septic Shock For The Obstetrician-Gynecologist PDFDocument20 pagesPlante-2016-Management of Sepsis and Septic Shock For The Obstetrician-Gynecologist PDFntnquynhproNo ratings yet
- Actualización-Endocarditis-bacteriana AmJMed 2020Document6 pagesActualización-Endocarditis-bacteriana AmJMed 2020msq.cv5919No ratings yet
- JCM 09 02870 v2Document9 pagesJCM 09 02870 v2Syaffa Sadida ZahraNo ratings yet
- Complicaciones de ElectroterpiaDocument3 pagesComplicaciones de ElectroterpiaSteeven TaipicañaNo ratings yet
- Publishing Case Reports: 8 Tips for SuccessDocument48 pagesPublishing Case Reports: 8 Tips for Successsryh2012No ratings yet
- Pediatric SepsisDocument16 pagesPediatric SepsisOsiithaa CañaszNo ratings yet
- Sepsisandsepticshock: Patrick J. MaloneyDocument18 pagesSepsisandsepticshock: Patrick J. MaloneyyoghaNo ratings yet
- Acquired RHD BestDocument95 pagesAcquired RHD BestauNo ratings yet
- A Cohort Study To Assess The New WHO Japanese Encephalitis Surveillance StandardsDocument9 pagesA Cohort Study To Assess The New WHO Japanese Encephalitis Surveillance StandardsarmankoassracunNo ratings yet
- COVID-19 InsigthDocument26 pagesCOVID-19 InsigthOmar FierroNo ratings yet
- Prescription of Antiviral Therapy After Herpes Zoster in General PracticeDocument7 pagesPrescription of Antiviral Therapy After Herpes Zoster in General PracticeAgaipNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument14 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- Is acute idiopathic pericarditis linked to recent viral illnessDocument6 pagesIs acute idiopathic pericarditis linked to recent viral illnessSarital BoronNo ratings yet
- Diagnosis and Treatment of Rheumatic FeverDocument4 pagesDiagnosis and Treatment of Rheumatic Fevernuwantha wickramasingheNo ratings yet
- Dengue JournalDocument4 pagesDengue JournalRohitKumarNo ratings yet
- Simple Clinical Indicators For Early Psoriatic Arthritis Detection.Document3 pagesSimple Clinical Indicators For Early Psoriatic Arthritis Detection.pancholarpancholarNo ratings yet
- 2525-Main Article Text (Blinded Article File) - 5250-2!10!20201009Document3 pages2525-Main Article Text (Blinded Article File) - 5250-2!10!20201009FihzanNo ratings yet
- Alzheimer's Disease Can Be Spared by Nonsteroidal Anti-Inflammatory DrugsDocument4 pagesAlzheimer's Disease Can Be Spared by Nonsteroidal Anti-Inflammatory DrugsAra Runa ConstellatiaNo ratings yet
- Clinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old ManDocument8 pagesClinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old MansamuelNo ratings yet
- I Human Case - EditedDocument5 pagesI Human Case - EditedFrancisNo ratings yet
- Artritis Séptica 27ago2023Document10 pagesArtritis Séptica 27ago2023José Alejandro Rivera JaramilloNo ratings yet
- Nihms940295 PDFDocument57 pagesNihms940295 PDFEkawatiNo ratings yet
- Communication CupDocument1 pageCommunication CupjoshNo ratings yet
- MED2 Tut1 Inflammation Healing Quiz NG 2021Document2 pagesMED2 Tut1 Inflammation Healing Quiz NG 2021joshNo ratings yet
- Drug FormularyDocument3 pagesDrug FormularyjoshNo ratings yet
- Ecase 07 - Tutorial 1 - 2021Document16 pagesEcase 07 - Tutorial 1 - 2021joshNo ratings yet
- ECase 08 - Tutorial 1 - 2021 Josh ThomasDocument15 pagesECase 08 - Tutorial 1 - 2021 Josh ThomasjoshNo ratings yet
- ECase 08 - Tutorial 1 - 2021 Josh ThomasDocument15 pagesECase 08 - Tutorial 1 - 2021 Josh ThomasjoshNo ratings yet
- Relation Between Diet and Kidney Disease Research PaperDocument4 pagesRelation Between Diet and Kidney Disease Research PaperjoshNo ratings yet
- Exercise and The BrainDocument19 pagesExercise and The BrainjoshNo ratings yet
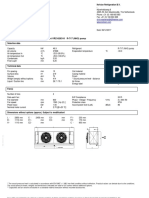
- GSL DIP Phase - 1 Cooler 45kWDocument1 pageGSL DIP Phase - 1 Cooler 45kWMuhasin PallikkalNo ratings yet
- A Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiDocument7 pagesA Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiShabir AhmadNo ratings yet
- ON Code (Aci 318-77) : Commentary Building Requirements For Reinforced ConcreteDocument132 pagesON Code (Aci 318-77) : Commentary Building Requirements For Reinforced ConcreteAzmi BazazouNo ratings yet
- MUSCULAR SYSTEM WORKSHEET Slides 1 To 4Document4 pagesMUSCULAR SYSTEM WORKSHEET Slides 1 To 4kwaiyuen ohnNo ratings yet
- AAB 075323 EPDM Waterproofing Membrane (For RC Roof Build-Up Inc. Insulation)Document3 pagesAAB 075323 EPDM Waterproofing Membrane (For RC Roof Build-Up Inc. Insulation)tewodrosNo ratings yet
- Altivar ATV61HU55N4 CatalogueDocument4 pagesAltivar ATV61HU55N4 CatalogueEugen Marius BadescuNo ratings yet
- Bipolar I Disorder Case ExampleDocument6 pagesBipolar I Disorder Case ExampleGrape JuiceNo ratings yet
- Tcgbutopia G8Document216 pagesTcgbutopia G8faffsNo ratings yet
- Cefiget-Range-Leaflet-PakistanDocument2 pagesCefiget-Range-Leaflet-PakistanZafran KhanNo ratings yet
- Bs. in P&O India. Syllabus 2010Document58 pagesBs. in P&O India. Syllabus 2010Priscila Arriagada PulgarNo ratings yet
- LEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019Document18 pagesLEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019kaito kurabaNo ratings yet
- Fundamentals of Wind EnergyDocument24 pagesFundamentals of Wind EnergyMas3odNo ratings yet
- Beneficiation of Cassiterite From Primary Tin OresDocument11 pagesBeneficiation of Cassiterite From Primary Tin OresSULMAGNo ratings yet
- Zooniverse Book 2022Document28 pagesZooniverse Book 2022Dr Pankaj DhussaNo ratings yet
- Final Seminar ReportDocument35 pagesFinal Seminar ReportHrutik BhandareNo ratings yet
- 2011 02 Huijben Spie Why Every Urea Plant Needs A Continuous NC Meter PDFDocument9 pages2011 02 Huijben Spie Why Every Urea Plant Needs A Continuous NC Meter PDFfawadintNo ratings yet
- Shangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Document2 pagesShangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Salma FarooqNo ratings yet
- Design of Temporary Floating Road for Construction SiteDocument6 pagesDesign of Temporary Floating Road for Construction SiteAnonymous hRWwL7pZnCNo ratings yet
- Ac+lic Lab Manual 2018-19Document76 pagesAc+lic Lab Manual 2018-19Samanvi SaatviNo ratings yet
- Exercitii AdjectivDocument3 pagesExercitii AdjectivFirma GSCNo ratings yet
- Empowerment Technologies: Quarter 3 - 8: Imaging and Design Fo R The Online Environment IDocument14 pagesEmpowerment Technologies: Quarter 3 - 8: Imaging and Design Fo R The Online Environment IShaira Jane Estrella UcolNo ratings yet
- CFD Answer KeyDocument12 pagesCFD Answer KeyRaahini IzanaNo ratings yet
- Regulation 1 Regulation 2 Regulation 3 Regulation 4 Regulation 5 Regulation 6 Regulation 7 Regulation 8 Regulation 9 AppendixDocument10 pagesRegulation 1 Regulation 2 Regulation 3 Regulation 4 Regulation 5 Regulation 6 Regulation 7 Regulation 8 Regulation 9 AppendixAnonymous 7gJ9alpNo ratings yet
- Kraby System 2018Document22 pagesKraby System 2018soga010178No ratings yet
- Ic M802 UDocument79 pagesIc M802 Uharis_fikriNo ratings yet
- IRIScan Book Executive 3 PDFDocument86 pagesIRIScan Book Executive 3 PDFssamplingNo ratings yet
- 2 1 Flash Klasa 6 Mod 1b Test ExtendedDocument4 pages2 1 Flash Klasa 6 Mod 1b Test ExtendedMonika Ciepłuch-Jarema100% (1)
- Flange Insulation Sets: Technical SpecificationDocument6 pagesFlange Insulation Sets: Technical SpecificationNor Azlan AwangNo ratings yet
- Siemens 810dDocument13 pagesSiemens 810dAdo ŠehićNo ratings yet
- MayankDocument38 pagesMayankmayank13430No ratings yet