You might also like
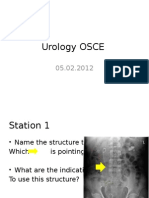
- Urology OSCEDocument9 pagesUrology OSCEJihad Anad75% (4)
- VZVXXXZVDocument342 pagesVZVXXXZVRahul GuptaNo ratings yet
- Sample Competency Assessment ToolDocument10 pagesSample Competency Assessment ToolHengkyNo ratings yet
- Ethnobotanical Important Plants Among THDocument12 pagesEthnobotanical Important Plants Among THJohn VillalbaNo ratings yet
- Parkinson DeseaseDocument35 pagesParkinson DeseaseNia SotoNo ratings yet
- Psychiatric Nursing: What Is Mental Health Disorder? SilenceDocument11 pagesPsychiatric Nursing: What Is Mental Health Disorder? SilenceJek Dela CruzNo ratings yet
- Photophobia: CausesDocument3 pagesPhotophobia: CausesmrscronnNo ratings yet
- Antiparkinson Drugs09Document39 pagesAntiparkinson Drugs09Gurveer ToorNo ratings yet
- ListApexHospitals2021 dc2021-0567Document4 pagesListApexHospitals2021 dc2021-0567Rey Coroña NardoNo ratings yet
- Anti Parkinson Drugs FinallDocument36 pagesAnti Parkinson Drugs FinallandrapradeshsseNo ratings yet
- Drug PresentationDocument32 pagesDrug PresentationManisha ShakyaNo ratings yet
- Parkinson's DiseaseDocument65 pagesParkinson's DiseaseGerald Resubal OriñaNo ratings yet
- Pharmacotherapy of Parkinson's DiseaseDocument66 pagesPharmacotherapy of Parkinson's DiseaseKenneth NuñezNo ratings yet
- Mayra Pagan: Pharmacology-NursingDocument50 pagesMayra Pagan: Pharmacology-NursingmayraNo ratings yet
- Triple SDEA Completed TemplateDocument7 pagesTriple SDEA Completed TemplateEman Moubarak50% (2)
- Golwala Medicine Book PDFDocument3 pagesGolwala Medicine Book PDFHesbon Momanyi67% (3)
- NCM 107A-Nursing Leadership and Managemen... (NCM 107A - Nursing Leadership & Management (Lecture) )Document32 pagesNCM 107A-Nursing Leadership and Managemen... (NCM 107A - Nursing Leadership & Management (Lecture) )Jek Dela CruzNo ratings yet
- Acupuncture PointsDocument14 pagesAcupuncture PointsJose Gregorio ParraNo ratings yet
- Anti ParkinsonismsDocument7 pagesAnti ParkinsonismsArslan SaeedNo ratings yet
- Parkinson Drug TherapyDocument20 pagesParkinson Drug Therapympl.raol50% (2)
- Drugs Used in Parkinsonism: Functional Circuitry Between The Cortex, Basal Ganglia, and ThalamusDocument5 pagesDrugs Used in Parkinsonism: Functional Circuitry Between The Cortex, Basal Ganglia, and ThalamusHamad AlshabiNo ratings yet
- Antiparkinson DrugsDocument19 pagesAntiparkinson DrugsSV SagarNo ratings yet
- Continum ParkinsonDocument14 pagesContinum Parkinsonfernando gonzalezNo ratings yet
- Chap 5 CNSDocument106 pagesChap 5 CNSKIDUS YAREDNo ratings yet
- Nursing - 1 AntiParkinsonian Drug - MehreenDocument35 pagesNursing - 1 AntiParkinsonian Drug - MehreenKhubaib KhanNo ratings yet
- Parkinson'sDisease DrugsDocument54 pagesParkinson'sDisease DrugstheintrovNo ratings yet
- Anti Parkinson Disease - PDF - Pharmacology - AssignmentDocument11 pagesAnti Parkinson Disease - PDF - Pharmacology - AssignmentMr HotmasterNo ratings yet
- Drugs That Cause and Drugs That Alleviate Parkinsonism: BY Prof. Mbah A.UDocument24 pagesDrugs That Cause and Drugs That Alleviate Parkinsonism: BY Prof. Mbah A.UtemitopeNo ratings yet
- Pharm - Chapter - 15 - Antiparkinson DrugsDocument44 pagesPharm - Chapter - 15 - Antiparkinson DrugsFeliciaDorghamNo ratings yet
- Movement DisordersDocument28 pagesMovement DisordersSheron MathewNo ratings yet
- ParkinsonismDocument18 pagesParkinsonismShivsharanNo ratings yet
- Anti-Parkinsonism DrugDocument15 pagesAnti-Parkinsonism Drugsaihjad pramaniNo ratings yet
- Movement DisordersDocument28 pagesMovement DisordersAhmad WaliNo ratings yet
- Anti ParkinsonDocument37 pagesAnti ParkinsonAkmal SafwanNo ratings yet
- CNS PNS DrugsDocument29 pagesCNS PNS DrugsMadel A. AlberioNo ratings yet
- Drug Therapy of ParkinsonismDocument28 pagesDrug Therapy of ParkinsonismZobayer AhmedNo ratings yet
- And Other Movement DisordersDocument38 pagesAnd Other Movement DisordersshravaniNo ratings yet
- PARKINSONSDocument82 pagesPARKINSONSCesarMatthewUlepMadriaNo ratings yet
- Drugs For Parkinson's DiseaseDocument43 pagesDrugs For Parkinson's DiseasesabaNo ratings yet
- Lect 3A - Other Drugs Act On The CNS - 29 Sept 2021Document49 pagesLect 3A - Other Drugs Act On The CNS - 29 Sept 2021Garry SoloanNo ratings yet
- Parkinson's Disease and TreatmentDocument13 pagesParkinson's Disease and Treatmentmaryam batoolNo ratings yet
- MILV8N8Document4 pagesMILV8N8garywall.ukNo ratings yet
- Antiparkinson Pharma 2020Document26 pagesAntiparkinson Pharma 2020Ida Bagus Putu SwabawaNo ratings yet
- Block I Posting, Pharmacology Lectures: Antiparkisonian DrugsDocument41 pagesBlock I Posting, Pharmacology Lectures: Antiparkisonian DrugsOdiete EfeNo ratings yet
- Medical Treatments For ParkinsonDocument4 pagesMedical Treatments For ParkinsonecwillNo ratings yet
- Block I Posting, Pharmacology Lectures: Dr. Aduragbenro AdedapoDocument47 pagesBlock I Posting, Pharmacology Lectures: Dr. Aduragbenro AdedapoOdiete EfeNo ratings yet
- 新泰醫院 家庭醫學科主治醫師 關鍵詞: Parkinson's disease, levodopa, dopamine agonistsDocument5 pages新泰醫院 家庭醫學科主治醫師 關鍵詞: Parkinson's disease, levodopa, dopamine agonistsChiu Chen LinNo ratings yet
- Levodopa 250mg + Carbidopa 25mg (Dopicar)Document10 pagesLevodopa 250mg + Carbidopa 25mg (Dopicar)ddandan_2No ratings yet
- Screenshot 2022-12-12 at 7.31.29 PMDocument16 pagesScreenshot 2022-12-12 at 7.31.29 PMshreshta reddy PalleNo ratings yet
- Antiparkinson Agents: Art Hupka, Ph.D. 2009Document52 pagesAntiparkinson Agents: Art Hupka, Ph.D. 2009Gurjot KaurNo ratings yet
- Antiepileptics PD 501Document27 pagesAntiepileptics PD 501SidraNo ratings yet
- Parkinson's DiseaseDocument24 pagesParkinson's Diseasejanemwanza003No ratings yet
- Anti-Parkinson AgentsDocument35 pagesAnti-Parkinson AgentsMutya XDNo ratings yet
- Dietitians Bestpracticeguideline PDFDocument12 pagesDietitians Bestpracticeguideline PDFCitra AuraNo ratings yet
- Right-Hand Tremor at Rest, WhichDocument47 pagesRight-Hand Tremor at Rest, WhichsyarintaadeninaNo ratings yet
- Antiparkinsons DrugsDocument19 pagesAntiparkinsons Drugs39 Nayan BhagatNo ratings yet
- Treatment of Epilepsy: Maha M. Saber, MD, MRCP (UK) Assistant Professor of Pharmacology, UOSDocument40 pagesTreatment of Epilepsy: Maha M. Saber, MD, MRCP (UK) Assistant Professor of Pharmacology, UOSSofiane TighiltNo ratings yet
- 00 Soal NeuroDocument4 pages00 Soal NeuroJasen ErickoNo ratings yet
- ParkinsonDocument9 pagesParkinsonTriNo ratings yet
- Dekinet Tablets: Use in PregnancyDocument3 pagesDekinet Tablets: Use in Pregnancyddandan_2No ratings yet
- Phenobarbital - DLF1 - PDFDocument5 pagesPhenobarbital - DLF1 - PDFMJANo ratings yet
- Anti Parkinsonism DrugsDocument8 pagesAnti Parkinsonism DrugsFaria Islam Juhi100% (1)
- HNS50 - Drugs Used For Neurodegenerative DiseasesDocument55 pagesHNS50 - Drugs Used For Neurodegenerative DiseasesJinyoungNo ratings yet
- 10-Antiparkinsonian and Spasmolytic AgentsDocument32 pages10-Antiparkinsonian and Spasmolytic Agentszeynep özdalNo ratings yet
- Drugs For Parkinson's DiseaseDocument52 pagesDrugs For Parkinson's DiseaseKAMALNo ratings yet
- Complications of Drug Therapy in Parkinson'sDocument15 pagesComplications of Drug Therapy in Parkinson'skaanchipatel02No ratings yet
- Drugs Used in ParkinsonismDocument16 pagesDrugs Used in ParkinsonismShahid HameedNo ratings yet
- Drugs Used in ParkinsonismDocument16 pagesDrugs Used in ParkinsonismShahid HameedNo ratings yet
- Fast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonFrom EverandFast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonNo ratings yet
- Fast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteFrom EverandFast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteNo ratings yet
- Pharmacology - Sept23Document23 pagesPharmacology - Sept23Jek Dela CruzNo ratings yet
- Safety Goals Business Plan: I. Executive SummaryDocument10 pagesSafety Goals Business Plan: I. Executive SummaryJek Dela CruzNo ratings yet
- Handout Endo - Sept24Document23 pagesHandout Endo - Sept24Jek Dela CruzNo ratings yet
- 10 Delacruz NeuroDocument4 pages10 Delacruz NeuroJek Dela CruzNo ratings yet
- A Case Study On Pulmonary Tuberculosis: Intensive PracticumDocument36 pagesA Case Study On Pulmonary Tuberculosis: Intensive PracticumJek Dela CruzNo ratings yet
- Intensive Practicum Official TemplateDocument4 pagesIntensive Practicum Official TemplateJek Dela CruzNo ratings yet
- Pulmonary Tuberculosis: Dela Cruz, JesfelDocument25 pagesPulmonary Tuberculosis: Dela Cruz, JesfelJek Dela CruzNo ratings yet
- 9 Delacruz PerfDocument4 pages9 Delacruz PerfJek Dela CruzNo ratings yet
- Case Studies On Major Concepts: Cellular AberrationDocument38 pagesCase Studies On Major Concepts: Cellular AberrationJek Dela CruzNo ratings yet
- 8 Delacruz CaDocument4 pages8 Delacruz CaJek Dela CruzNo ratings yet
- Case Studies On Major Concepts: Emergency and TraumaDocument37 pagesCase Studies On Major Concepts: Emergency and TraumaJek Dela CruzNo ratings yet
- Case Studies On Major Concepts: PerfusionDocument37 pagesCase Studies On Major Concepts: PerfusionJek Dela CruzNo ratings yet
- 5 - Fluid and ElectrolyteDocument37 pages5 - Fluid and ElectrolyteJek Dela CruzNo ratings yet
- 6 - Infection and InflammationDocument37 pages6 - Infection and InflammationJek Dela CruzNo ratings yet
- Case Studies On Major Concepts: NeurologicalDocument37 pagesCase Studies On Major Concepts: NeurologicalJek Dela CruzNo ratings yet
- 4 - Acute Biologic CrisisDocument37 pages4 - Acute Biologic CrisisJek Dela CruzNo ratings yet
- Alcohol Treatment ProgramDocument2 pagesAlcohol Treatment ProgramJek Dela CruzNo ratings yet
- Case Studies On Major Concepts: MetabolismDocument37 pagesCase Studies On Major Concepts: MetabolismJek Dela CruzNo ratings yet
- Case Studies On Major Concepts: OxygenationDocument37 pagesCase Studies On Major Concepts: OxygenationJek Dela CruzNo ratings yet
- Responses, And/or Inability To Use Available ResourcesDocument2 pagesResponses, And/or Inability To Use Available ResourcesJek Dela CruzNo ratings yet
- 1 - Perception and CoordinationDocument37 pages1 - Perception and CoordinationJek Dela CruzNo ratings yet
- Dela CruzDocument1 pageDela CruzJek Dela CruzNo ratings yet
- Kode Kode DiagnosaDocument4 pagesKode Kode DiagnosaSibintang 123pagarNo ratings yet
- DAFTAR PUSTAKA PanhipopituitarismDocument2 pagesDAFTAR PUSTAKA PanhipopituitarismNoEr FitRiaNo ratings yet
- Typhoid Fever para PresentDocument23 pagesTyphoid Fever para PresentGino Al Ballano BorinagaNo ratings yet
- Medical Emergency Preparedness / First Aid in Trauma SituationsDocument66 pagesMedical Emergency Preparedness / First Aid in Trauma Situations1pallabNo ratings yet
- Assignment 2Document8 pagesAssignment 2akincade999No ratings yet
- Crossword ExamDocument1 pageCrossword Examtwilight_6teenNo ratings yet
- Aborsion: Spontaneou SDocument214 pagesAborsion: Spontaneou Sorkaido berisha (Addisu)No ratings yet
- Risk Management in Medical LaboratoriesDocument32 pagesRisk Management in Medical Laboratoriesapanisile14142No ratings yet
- Current Trends in The Popular Sector Traditional Medicine in Sri LankaDocument10 pagesCurrent Trends in The Popular Sector Traditional Medicine in Sri Lankammarikar27No ratings yet
- REP19 AMReDocument32 pagesREP19 AMRe3utiaNo ratings yet
- Harrell First Amended Complaint - (To FILE)Document38 pagesHarrell First Amended Complaint - (To FILE)John Del SignoreNo ratings yet
- ImpulogDocument31 pagesImpulogNimesh ModiNo ratings yet
- Ebook Ebook PDF Operative Techniques Shoulder and Elbow Surgery 2Nd Edition All Chapter PDF Docx KindleDocument41 pagesEbook Ebook PDF Operative Techniques Shoulder and Elbow Surgery 2Nd Edition All Chapter PDF Docx Kindleyolanda.gilliam435100% (16)
- Internship Reflection PaperDocument7 pagesInternship Reflection Paperapi-518707218No ratings yet
- Dialysis and Disasters PresentationDocument21 pagesDialysis and Disasters Presentationapi-24755251No ratings yet
- 2 Ract 20140411Document33 pages2 Ract 20140411Richard Thodé JrNo ratings yet
- Fundamentals of Critical Care-A Textbook For Nursing and Healthcare Students (Oct 10, 2022) - (1119783259) - (Wiley-Blackwell) 1st Edition Ian PeateDocument68 pagesFundamentals of Critical Care-A Textbook For Nursing and Healthcare Students (Oct 10, 2022) - (1119783259) - (Wiley-Blackwell) 1st Edition Ian Peateoscar.draper548100% (9)
- SDM Dental College MDS Admission Procedure 1 1Document2 pagesSDM Dental College MDS Admission Procedure 1 1isteNo ratings yet
- Mechanisms, Causes, and Evaluation of Orthostatic Hypotension - UpToDateDocument20 pagesMechanisms, Causes, and Evaluation of Orthostatic Hypotension - UpToDateCipriano Di MauroNo ratings yet
- Simulation-Consent For SurgicalDocument2 pagesSimulation-Consent For SurgicalMargaret Barco DeanesNo ratings yet
- DSM 5 Autism Spectrum Disorder Fact SheetDocument2 pagesDSM 5 Autism Spectrum Disorder Fact SheetMario MendozaNo ratings yet