You might also like
- Application of Lean Approaches and Techniques in An Automotive CompanyDocument8 pagesApplication of Lean Approaches and Techniques in An Automotive CompanyAchraf adenasNo ratings yet
- Application of Value Stream Mapping and 5s For Redraw Machine in Pump Industry IJERTCONV5IS07011Document6 pagesApplication of Value Stream Mapping and 5s For Redraw Machine in Pump Industry IJERTCONV5IS07011Ibrahim SkakriNo ratings yet
- Slidesharespaghettichart 170609205825Document12 pagesSlidesharespaghettichart 170609205825Ibrahim SkakriNo ratings yet
- The Spaghetti DiagramDocument21 pagesThe Spaghetti DiagramBoamina Balondona AurelienNo ratings yet
- Lean Warehousing: A Case Study of A Greek Warehouse: Master's Thesis (30 Credits)Document75 pagesLean Warehousing: A Case Study of A Greek Warehouse: Master's Thesis (30 Credits)Ibrahim SkakriNo ratings yet
- Lean Warehouse Management PaperDocument33 pagesLean Warehouse Management PaperIbrahim SkakriNo ratings yet
- Improving Efficiency in A Hybrid Warehouse: A Case Study Improving Efficiency in A Hybrid Warehouse: A Case StudyDocument11 pagesImproving Efficiency in A Hybrid Warehouse: A Case Study Improving Efficiency in A Hybrid Warehouse: A Case StudyIbrahim SkakriNo ratings yet
- Lean principles for improving warehouse efficiencyDocument5 pagesLean principles for improving warehouse efficiencyYosua ArmandNo ratings yet
- FP Lean Warehouse OperationsDocument8 pagesFP Lean Warehouse OperationsIbrahim SkakriNo ratings yet
- New Strategy For Warehouse Optimization - Lean WarehousingDocument7 pagesNew Strategy For Warehouse Optimization - Lean WarehousingBennet RajkumarNo ratings yet
- Applying Lean Concepts in A Warehouse Operation: Related PapersDocument7 pagesApplying Lean Concepts in A Warehouse Operation: Related PapersIbrahim SkakriNo ratings yet
- Implementation of Lean Warehousing To Reduce The Level of Returns in A Distribution CompanyDocument5 pagesImplementation of Lean Warehousing To Reduce The Level of Returns in A Distribution CompanyIbrahim SkakriNo ratings yet
- The Role and Importance of Lean Tools in Warehouse ManagementDocument8 pagesThe Role and Importance of Lean Tools in Warehouse ManagementIbrahim SkakriNo ratings yet
- Implementation of Lean Warehousing To Reduce The Level of Returns in A Distribution CompanyDocument5 pagesImplementation of Lean Warehousing To Reduce The Level of Returns in A Distribution CompanyIbrahim SkakriNo ratings yet
- Improving Road Transport Operations Through Lean Thinking: A Case StudyDocument25 pagesImproving Road Transport Operations Through Lean Thinking: A Case StudyIbrahim SkakriNo ratings yet
- Platform Real Estate: Theory and Practice of New Urban Real Estate MarketsDocument29 pagesPlatform Real Estate: Theory and Practice of New Urban Real Estate MarketsIbrahim SkakriNo ratings yet
- Continuous Improvement To Create Value: Warehouse Management in A Telecommunications CompanyDocument8 pagesContinuous Improvement To Create Value: Warehouse Management in A Telecommunications CompanyIbrahim SkakriNo ratings yet
- 5S Lean Tool, Value Stream Mapping and Warehouse Performance: Conceptual FrameworkDocument4 pages5S Lean Tool, Value Stream Mapping and Warehouse Performance: Conceptual FrameworkIbrahim SkakriNo ratings yet
- Maina-Effect of Digital Marketing Tools On Performance of Businesses in Real Estate Sector in Nairobi CountyDocument86 pagesMaina-Effect of Digital Marketing Tools On Performance of Businesses in Real Estate Sector in Nairobi CountyIbrahim SkakriNo ratings yet
- Sustainability 10 03142 v2 PDFDocument44 pagesSustainability 10 03142 v2 PDFRajat YadavNo ratings yet
- Digital Marketing and ItsImpulsivenessinDocument7 pagesDigital Marketing and ItsImpulsivenessinIbrahim SkakriNo ratings yet
- Application of Lean Approaches and Techniques in An Automotive CompanyDocument8 pagesApplication of Lean Approaches and Techniques in An Automotive CompanyAchraf adenasNo ratings yet
- Irjet A Study On The Impact of Online MaDocument3 pagesIrjet A Study On The Impact of Online MaIbrahim SkakriNo ratings yet
- Improving Pharmaceutical Warehouse Supply Chain Lead Time - From Production To Cross-DockingDocument6 pagesImproving Pharmaceutical Warehouse Supply Chain Lead Time - From Production To Cross-DockingIbrahim SkakriNo ratings yet
- Site AuditDocument1 pageSite AuditIbrahim SkakriNo ratings yet
- Implementation of Lean Techniques For Sustainable Workflow Process in Indian Motor Manufacturing UnitDocument9 pagesImplementation of Lean Techniques For Sustainable Workflow Process in Indian Motor Manufacturing Unithcshipra007No ratings yet
- Improving Efficiency in A Hybrid Warehouse: A Case Study Improving Efficiency in A Hybrid Warehouse: A Case StudyDocument11 pagesImproving Efficiency in A Hybrid Warehouse: A Case Study Improving Efficiency in A Hybrid Warehouse: A Case StudyIbrahim SkakriNo ratings yet
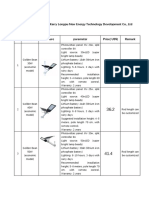
- Split Solar Light and Price ListDocument9 pagesSplit Solar Light and Price ListIbrahim SkakriNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Asia Ghee Mill ReportDocument27 pagesAsia Ghee Mill ReportHafiz AbdulwahabNo ratings yet
- Lesson 2 of FirstDocument18 pagesLesson 2 of FirstMYRRH TRAINNo ratings yet
- Product and Service Design ReviewerDocument7 pagesProduct and Service Design ReviewerFrue LoveNo ratings yet
- L.L.Bean, Inc.: (Item Forecasting and Inventory Management)Document9 pagesL.L.Bean, Inc.: (Item Forecasting and Inventory Management)Swarnajit SahaNo ratings yet
- Working CapitalDocument75 pagesWorking CapitalJayavardhan 2B1 8No ratings yet
- Logistics Role in Business and Economy DimensionsDocument54 pagesLogistics Role in Business and Economy DimensionsCipaidunkNo ratings yet
- Abas Erp Production - Eng PDFDocument28 pagesAbas Erp Production - Eng PDFDavid Tan100% (1)
- Samsung's Global Supply Chain ManagementDocument30 pagesSamsung's Global Supply Chain ManagementHương LýNo ratings yet
- Goal: Book SummaryDocument5 pagesGoal: Book SummaryAnand Prakash JhaNo ratings yet
- (ACCT2010) (2017) (F) Midterm In5mue0 38655Document4 pages(ACCT2010) (2017) (F) Midterm In5mue0 38655Pak HoNo ratings yet
- Bhel JitDocument4 pagesBhel Jitswaroopce100% (2)
- Acccob2 Reflection #2Document8 pagesAcccob2 Reflection #2asiacrisostomoNo ratings yet
- Ebook Starting A Business 101 PDFDocument44 pagesEbook Starting A Business 101 PDFusateNo ratings yet
- Ax2012R3 & R2 & 2009 SP1 HotfixlistDocument723 pagesAx2012R3 & R2 & 2009 SP1 HotfixlistTariq RafiqueNo ratings yet
- Asset Management SoftwareDocument6 pagesAsset Management SoftwareMahendran MunuNo ratings yet
- Module 1-1 Cost Accounting FundamentalsDocument9 pagesModule 1-1 Cost Accounting FundamentalsClaire BarbaNo ratings yet
- Toyota's Impact on Global Supply ChainsDocument20 pagesToyota's Impact on Global Supply Chainsshubo palitNo ratings yet
- Project Management Exam QuestionsDocument29 pagesProject Management Exam QuestionsMukund KoiralaNo ratings yet
- QuizDocument12 pagesQuizFarid saidNo ratings yet
- Time Management: Dr. Saleh MubarakDocument89 pagesTime Management: Dr. Saleh MubarakTriet TruongNo ratings yet
- A 4 Operational Due Diligence Report TemplateDocument29 pagesA 4 Operational Due Diligence Report TemplateDickson Allela100% (1)
- What Is The Role of JIT and Lean in Inventory ManagementDocument16 pagesWhat Is The Role of JIT and Lean in Inventory ManagementhuleNo ratings yet
- Accounting For Manufacturing ConcernDocument2 pagesAccounting For Manufacturing ConcernAhmed MemonNo ratings yet
- Financial Management 1 ProblemsDocument12 pagesFinancial Management 1 ProblemsXytusNo ratings yet
- UNIT-1 Planning and Organising The House Keeping Department The Planning ProcessDocument72 pagesUNIT-1 Planning and Organising The House Keeping Department The Planning Processakshay ranaNo ratings yet
- Ch11Document20 pagesCh11raamNo ratings yet
- Introduction To ManufacturingDocument48 pagesIntroduction To ManufacturingSyakir ImanNo ratings yet
- Strictly NO ERASURES Multiple Choice TestDocument12 pagesStrictly NO ERASURES Multiple Choice TestUy SamuelNo ratings yet
- Operations Management: William J. StevensonDocument40 pagesOperations Management: William J. StevensonmadihaNo ratings yet
- CLTD Ecm 2.0Document36 pagesCLTD Ecm 2.0Sahara SneedanNo ratings yet