You might also like
- Systematic Review and Meta-Analysis of TracheostomyDocument12 pagesSystematic Review and Meta-Analysis of Tracheostomycelma44No ratings yet
- Laryngeal Complications of COVID-19Document8 pagesLaryngeal Complications of COVID-19Mariana BarrosNo ratings yet
- Normal and Pathological Bronchial Semiology: A Visual ApproachFrom EverandNormal and Pathological Bronchial Semiology: A Visual ApproachPierre Philippe BaldeyrouNo ratings yet
- Bilateral Vocal Fold Immobility: A 13 Year Review of Etiologies, Management and The Utility of The Empey IndexDocument7 pagesBilateral Vocal Fold Immobility: A 13 Year Review of Etiologies, Management and The Utility of The Empey IndexRadita Dwihaning PutriNo ratings yet
- Lung Transplantation: Evolving Knowledge and New HorizonsFrom EverandLung Transplantation: Evolving Knowledge and New HorizonsGanesh RaghuNo ratings yet
- Mouth Care and VAPDocument8 pagesMouth Care and VAPEmily HazeltonNo ratings yet
- Crowson2019 Article VocalFoldParalysisParesisAsAMaDocument12 pagesCrowson2019 Article VocalFoldParalysisParesisAsAMaAnna AgenteNo ratings yet
- Jurnal ArdsDocument5 pagesJurnal Ardsdani yan sNo ratings yet
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Ear, Nose, and Throat Description at Acute Stage and After RemissionDocument6 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis Ear, Nose, and Throat Description at Acute Stage and After RemissionElsa Giatri SiradjNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- 2011 - Preoperative Endoscopic Airway Examination (PEAE) Provides Superior Airway Information and May Reduce The Use of Unnecessary Awake Ion - MylenaDocument6 pages2011 - Preoperative Endoscopic Airway Examination (PEAE) Provides Superior Airway Information and May Reduce The Use of Unnecessary Awake Ion - MylenaMirella Andraous100% (1)
- 1807 5932 Clin 75 E2021Document2 pages1807 5932 Clin 75 E2021Claudia Lorena MedinaNo ratings yet
- Clinical Signs Commonly Seen On Ent Examination of Symptomatic Active Covid-19 Patients in Our Tertiary Care CentreDocument6 pagesClinical Signs Commonly Seen On Ent Examination of Symptomatic Active Covid-19 Patients in Our Tertiary Care CentreIJAR JOURNALNo ratings yet
- Prevencion de La Neummonia PostDocument9 pagesPrevencion de La Neummonia PostDiana SalinasNo ratings yet
- The Management of Ingested Foreign Bodies in An Ear, Nose, and Throat Emergency Unit: Prospective Study of 204 CasesDocument7 pagesThe Management of Ingested Foreign Bodies in An Ear, Nose, and Throat Emergency Unit: Prospective Study of 204 CasesheribertusNo ratings yet
- Timing of Tracheostomy For Prolonged Respiratory Wean in Critically Ill Coronavirus Disease 2019 Patients A Machine Learning ApproachDocument9 pagesTiming of Tracheostomy For Prolonged Respiratory Wean in Critically Ill Coronavirus Disease 2019 Patients A Machine Learning ApproachDewa OkaNo ratings yet
- Otolaryngological Manifestations in Hiv Infected Patients Tehran Iran 2155 6113.1000160Document4 pagesOtolaryngological Manifestations in Hiv Infected Patients Tehran Iran 2155 6113.1000160Adhelline RansunNo ratings yet
- UK cystic fibrosis patients prefer forced techniques and oscillating PEP for airway clearanceDocument25 pagesUK cystic fibrosis patients prefer forced techniques and oscillating PEP for airway clearancePaula UrsuNo ratings yet
- Videolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosDocument2 pagesVideolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosHugo Robles GómezNo ratings yet
- The OPERA TriaDocument7 pagesThe OPERA TriackeshavaNo ratings yet
- %pediatric TracheostomyDocument25 pages%pediatric TracheostomyFabian Camelo OtorrinoNo ratings yet
- Day-Case Stapes Surgery: Day-Case Versus Inpatient Stapes Surgery For Otosclerosis: A Randomized Controlled TrialDocument7 pagesDay-Case Stapes Surgery: Day-Case Versus Inpatient Stapes Surgery For Otosclerosis: A Randomized Controlled TrialNurul Khairiyah AmriNo ratings yet
- Early View: A Randomised Trial of High-Flow Nasal Cannula in Infants With Moderate BronchiolitisDocument28 pagesEarly View: A Randomised Trial of High-Flow Nasal Cannula in Infants With Moderate BronchiolitisutamiprakosoNo ratings yet
- Proceedings of Singapore Healthcare 2016 Wong 19 26Document8 pagesProceedings of Singapore Healthcare 2016 Wong 19 26Aristiyan LuthfiNo ratings yet
- Airway Volume Changes After Orthognathic Surgery in Patients With Down SyndromeDocument14 pagesAirway Volume Changes After Orthognathic Surgery in Patients With Down SyndrometamisatnamNo ratings yet
- 1 s2.0 S2095881118300611 Main 2Document5 pages1 s2.0 S2095881118300611 Main 2Delia RasmawatiNo ratings yet
- Protocol 2Document14 pagesProtocol 2Hamid RazaNo ratings yet
- 10.1002@lary.28626 EngDocument7 pages10.1002@lary.28626 EngRima Fairuuz PutriNo ratings yet
- High Flow Oxygen Therapy V Standard Care in InfantsDocument5 pagesHigh Flow Oxygen Therapy V Standard Care in InfantsJaque ArandaNo ratings yet
- Piskin Et Al-2014-Gerodontology PDFDocument6 pagesPiskin Et Al-2014-Gerodontology PDFGonzalo Báez VNo ratings yet
- (2013) Surgical Treatment of Severe EpistaxisDocument6 pages(2013) Surgical Treatment of Severe EpistaxisBang mantoNo ratings yet
- C 8 F 0 CF 2 F 9 C 13052842 DDocument11 pagesC 8 F 0 CF 2 F 9 C 13052842 DDewi Ji YongNo ratings yet
- Skoretz 2014Document8 pagesSkoretz 2014Gonzalo FragaNo ratings yet
- Aex 091Document9 pagesAex 091enriquegarciagalianaNo ratings yet
- 2018 Article 50Document10 pages2018 Article 50miss betawiNo ratings yet
- Sushma Thimmaiah KanakalakshmiDocument12 pagesSushma Thimmaiah KanakalakshmiBilly Aditya PratamaNo ratings yet
- Chest Physiotherapy in Children With Acute Bacterial PneumoniaDocument10 pagesChest Physiotherapy in Children With Acute Bacterial PneumoniaEka BagaskaraNo ratings yet
- Transbronchial Biopsy and Lavage in Diagnosing Diffuse Lung DiseaseDocument8 pagesTransbronchial Biopsy and Lavage in Diagnosing Diffuse Lung DiseasePandu Putra Wijaya RestaNo ratings yet
- Otolaryngology ComplicacionDocument7 pagesOtolaryngology ComplicacionYuriko Castro SanchezNo ratings yet
- 2021 Article 2410Document7 pages2021 Article 2410sibel yıldırımNo ratings yet
- Perawatan Intensif (IPI) Di Rumah Sakit-Rumah SakitDocument7 pagesPerawatan Intensif (IPI) Di Rumah Sakit-Rumah SakitCandra KurniatiNo ratings yet
- Original Article: Key WordsDocument9 pagesOriginal Article: Key WordsykommNo ratings yet
- HFNCDocument10 pagesHFNCDollenz Maldonado Natalie CamilaNo ratings yet
- Abstracts COMAPI 2014 IJMSDocument20 pagesAbstracts COMAPI 2014 IJMSfelipetheNo ratings yet
- GR Up: To Study The Diagnostic Yield of Medical Thoracoscopy in Patients With Pleural Effusion of Undetermined EtiologyDocument45 pagesGR Up: To Study The Diagnostic Yield of Medical Thoracoscopy in Patients With Pleural Effusion of Undetermined EtiologyChetan DhobleNo ratings yet
- Throat and Nasal Swabs For Molecular Detection of Respiratory Viruses in Acute PharyngitisDocument4 pagesThroat and Nasal Swabs For Molecular Detection of Respiratory Viruses in Acute PharyngitisFriskyShandy BadiNo ratings yet
- Lust StudyDocument7 pagesLust Studyadrianoneto60No ratings yet
- 01585-2021 FullDocument156 pages01585-2021 FullywtmyxpezickztrkcfNo ratings yet
- Art 12Document8 pagesArt 12Gabriela GarciaNo ratings yet
- Application of High-Fow Nasal CannulaDocument7 pagesApplication of High-Fow Nasal CannulaCLAUDIANo ratings yet
- Airway Management in Deep Neck InfectionsDocument1 pageAirway Management in Deep Neck InfectionsAlief Abni BernindraNo ratings yet
- 1-s2.0-S0749070424000071Document18 pages1-s2.0-S0749070424000071أركان هيلث Arkan healthNo ratings yet
- Otolaryngologist PPE Recommendations for COVID-19 PatientsDocument11 pagesOtolaryngologist PPE Recommendations for COVID-19 Patientsayuines lassyaniNo ratings yet
- Early View: High-Flow Nasal Cannula For COVID-19 Patients: Low Risk of Bio-Aerosol DispersionDocument9 pagesEarly View: High-Flow Nasal Cannula For COVID-19 Patients: Low Risk of Bio-Aerosol DispersionSekarNo ratings yet
- 2022-10# (PEERJ) RR in ECMODocument17 pages2022-10# (PEERJ) RR in ECMOjycntuNo ratings yet
- Children: Nebulizer Care and Inhalation Technique in Children With Cystic FibrosisDocument9 pagesChildren: Nebulizer Care and Inhalation Technique in Children With Cystic FibrosisyukihannaNo ratings yet
- RESPIRATORIODocument9 pagesRESPIRATORIOGloria BarriaNo ratings yet
- Post-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesDocument6 pagesPost-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesSoniJfreeNo ratings yet
- GJHS 6 221Document5 pagesGJHS 6 221Teuku FaisalNo ratings yet
- Jurnal Covid 2Document10 pagesJurnal Covid 2Elliot AndersonNo ratings yet
- Oropharyngeal Dysphagia and Aspiration Pneumonia Following Coronavirus Disease 2019: A Case ReportDocument4 pagesOropharyngeal Dysphagia and Aspiration Pneumonia Following Coronavirus Disease 2019: A Case ReportClaudia LorenaNo ratings yet
- Postintubation Dysphagia During COVID 19 Outbreak Contemporary ReviewDocument9 pagesPostintubation Dysphagia During COVID 19 Outbreak Contemporary ReviewvaleperoneNo ratings yet
- ParkinsonDocument9 pagesParkinsonIsabela FiuzaNo ratings yet
- ParkinsonDocument9 pagesParkinsonIsabela FiuzaNo ratings yet
- Parkinson TerapiaDocument13 pagesParkinson TerapiaIsabela FiuzaNo ratings yet
- Lesson Plan Nephrotic SyndromeDocument9 pagesLesson Plan Nephrotic SyndromeEllen Angel50% (2)
- The Dental Plaque Biofilm MatrixDocument25 pagesThe Dental Plaque Biofilm MatrixTasha FarahNo ratings yet
- Case Study Ischemic Heart DiseaseDocument16 pagesCase Study Ischemic Heart DiseaseRawan KhateebNo ratings yet
- Aida Amaliya - EssayDocument2 pagesAida Amaliya - EssayAida AmaliyaNo ratings yet
- DefibrillationDocument4 pagesDefibrillationNeha BhardwajNo ratings yet
- Fracture Healing - Basic Science - Orthobullets PDFDocument2 pagesFracture Healing - Basic Science - Orthobullets PDFMelAcostaNo ratings yet
- Radiobiology For The Radiologist 8th Edition Ebook PDFDocument61 pagesRadiobiology For The Radiologist 8th Edition Ebook PDFroy.mula622100% (40)
- ZOOL 143 Topic 6 Diseases Assosiated With HIV and AIDSDocument9 pagesZOOL 143 Topic 6 Diseases Assosiated With HIV and AIDSnattydreadfathelahNo ratings yet
- PROBLEM PRIORITY SETTING (Acob)Document3 pagesPROBLEM PRIORITY SETTING (Acob)Audrey Ann AcobNo ratings yet
- Parkinsons Disease Rating Scales A Literature RevDocument20 pagesParkinsons Disease Rating Scales A Literature RevIna Gorodețchi-DidîcNo ratings yet
- Ophthalmology 2Document235 pagesOphthalmology 2yididiyagirma30No ratings yet
- Mule AaDocument37 pagesMule AaShabaka KashataNo ratings yet
- Biochemistry Papers MSUDocument20 pagesBiochemistry Papers MSUShiv BhattNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- CBCR Joint Pain Student VersionDocument4 pagesCBCR Joint Pain Student VersionNika GianashviliNo ratings yet
- Whole Abdomen (Male)Document48 pagesWhole Abdomen (Male)Eftekharul IslamNo ratings yet
- Perioperative nursing considerationsDocument9 pagesPerioperative nursing considerationsKoleen Kirsten100% (1)
- 2022醫療急救 無線電醫療作業Document2 pages2022醫療急救 無線電醫療作業Yu-ting FengNo ratings yet
- Mental Health Consequences of Exercise WithdrawalDocument8 pagesMental Health Consequences of Exercise WithdrawaljasonNo ratings yet
- Rhenock, Sikkim Village ReportDocument101 pagesRhenock, Sikkim Village Reportankitsaxena88No ratings yet
- Covid Letter - North Peace Seniors HousingDocument2 pagesCovid Letter - North Peace Seniors HousingAlaskaHighwayNewsNo ratings yet
- Mushroom Production Technologies PDFDocument5 pagesMushroom Production Technologies PDFPruthwi RajNo ratings yet
- GCSE History Britain: Health and The People, C1000-Present DayDocument30 pagesGCSE History Britain: Health and The People, C1000-Present DayAniqah ShujaatNo ratings yet
- EPPP PRACTICE ExamDocument22 pagesEPPP PRACTICE Examh58qk7h6d2No ratings yet
- NCLEX-RN - REVIEW - NOTES.2018-2019 by Saeid AskariDocument150 pagesNCLEX-RN - REVIEW - NOTES.2018-2019 by Saeid Askarireza babaAli100% (1)
- Ecg For The Exam-Score 2020Document17 pagesEcg For The Exam-Score 2020prasannasimhaNo ratings yet
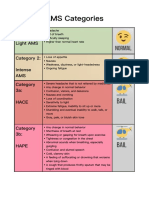
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Pedia Prof - OamilDocument147 pagesPedia Prof - OamilOne Click Online ShopNo ratings yet
- Ayurveda, YogaDocument34 pagesAyurveda, Yogayandi permanaNo ratings yet
- Zinobacilly Final TrainingDocument12 pagesZinobacilly Final TrainingShima ElshewyNo ratings yet