You might also like
- Mechanics of Solids by Sadhu Singhpdf Ebook and Ma PDFDocument1 pageMechanics of Solids by Sadhu Singhpdf Ebook and Ma PDFNeeraj Janghu0% (2)
- Grade 12 marketing principles course outlineDocument4 pagesGrade 12 marketing principles course outlineE-dlord M-alabanan100% (3)
- Sample Final Exam Larkin AnswersDocument18 pagesSample Final Exam Larkin AnswersLovejot SinghNo ratings yet
- 1 s2.0 S0899707121004113 MainDocument15 pages1 s2.0 S0899707121004113 MainJulian Rodriguez CelyNo ratings yet
- Bulbo-Medullary Ependymoma in An Adult: Case ReportDocument6 pagesBulbo-Medullary Ependymoma in An Adult: Case ReportIJAR JOURNALNo ratings yet
- TMP 33 BFDocument6 pagesTMP 33 BFFrontiersNo ratings yet
- ARTCICLEDocument7 pagesARTCICLErosa mendozaNo ratings yet
- Epidermoid Cysts TNEDocument10 pagesEpidermoid Cysts TNEbello_england_209552No ratings yet
- (10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesDocument9 pages(10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesasiyazaidiaNo ratings yet
- Hemagioma SCDocument5 pagesHemagioma SCCelebre MualabaNo ratings yet
- Medip, IJRMS-7729 ODocument7 pagesMedip, IJRMS-7729 ORagupathi MNo ratings yet
- Craniofacial Encephalocele: Updates On Management: Amelia Alberts, Brandon Lucke-WoldDocument13 pagesCraniofacial Encephalocele: Updates On Management: Amelia Alberts, Brandon Lucke-Woldhidayat adi putraNo ratings yet
- Solitary Plasmacytoma of The Thoracolumbar Spine A Rare Cas - 2022 - InterdisciDocument5 pagesSolitary Plasmacytoma of The Thoracolumbar Spine A Rare Cas - 2022 - Interdiscib00403007No ratings yet
- Imaging Findings of Intraventricular and Ependymal LesionsDocument16 pagesImaging Findings of Intraventricular and Ependymal Lesionsanggi abNo ratings yet
- Surgical Removal of Spinal Cord TumorsDocument8 pagesSurgical Removal of Spinal Cord TumorsLuwiNo ratings yet
- Cervical Sympathetic Chain Ganglioneuroma: Case Report and Review of LiteratureDocument4 pagesCervical Sympathetic Chain Ganglioneuroma: Case Report and Review of LiteratureIOSR Journal of PharmacyNo ratings yet
- Giant Thoracolumbar Extradural Arachnoid Cyst A CaDocument6 pagesGiant Thoracolumbar Extradural Arachnoid Cyst A Cailmiah neurologiNo ratings yet
- AsianJNeurosurg8121-7546405 205744Document8 pagesAsianJNeurosurg8121-7546405 205744WildaHanimNo ratings yet
- Meningioma With Cystic Change Mimicking Hemangioblastoma: SciencedirectDocument5 pagesMeningioma With Cystic Change Mimicking Hemangioblastoma: SciencedirectKhương Hà NguyễnNo ratings yet
- Surgical Outcomes of Cerebral CavernomasDocument12 pagesSurgical Outcomes of Cerebral CavernomasYovanka Naryai ManuhutuNo ratings yet
- Spinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SDocument3 pagesSpinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SRonald QuezadaNo ratings yet
- 690 FullDocument8 pages690 Fulldanielalexandersinaga.xiiipa2No ratings yet
- A Case Seriesof Neuroendocrine Tumours in Appendix: Incidental FindingsDocument7 pagesA Case Seriesof Neuroendocrine Tumours in Appendix: Incidental FindingsIJAR JOURNALNo ratings yet
- Endoscopic Endonasal Reconstruction of Anterior Skull Base Defects What Factors Really Affect The OutcomesDocument8 pagesEndoscopic Endonasal Reconstruction of Anterior Skull Base Defects What Factors Really Affect The OutcomesSanooj SeyedNo ratings yet
- ContentsDocument3 pagesContentsNaim CalilNo ratings yet
- Hannoun 2021Document4 pagesHannoun 2021mahaaNo ratings yet
- Embolización Angiografica ArtDocument5 pagesEmbolización Angiografica ArtIsamar AlvarezNo ratings yet
- Cystic Lesions of The Brain A Classification Based On PathogenesisDocument16 pagesCystic Lesions of The Brain A Classification Based On Pathogenesisveerraju tvNo ratings yet
- Songcharoen 1995Document5 pagesSongcharoen 1995Le Manh ThuongNo ratings yet
- Chaussemy 2015Document4 pagesChaussemy 2015Kimé RyNo ratings yet
- BJUI Compass - 2020 - Anderson - Subinguinal Orchiectomy A Minimally Invasive Approach To Open SurgeryDocument5 pagesBJUI Compass - 2020 - Anderson - Subinguinal Orchiectomy A Minimally Invasive Approach To Open SurgeryKaroo_123No ratings yet
- Spinal Tumors ArticleDocument5 pagesSpinal Tumors ArticleMariaLakhaniNo ratings yet
- Spinal Tumour Surgery OutcomesDocument5 pagesSpinal Tumour Surgery OutcomesNouman Safdar AliNo ratings yet
- Pictorial Essay of Cranial Nerves Lesions On MRI Our ExperienceDocument10 pagesPictorial Essay of Cranial Nerves Lesions On MRI Our ExperienceAamir YousufNo ratings yet
- 1-s2.0-S1878875018300159-mainDocument9 pages1-s2.0-S1878875018300159-mainAlexandreNo ratings yet
- Raval PDFDocument5 pagesRaval PDFdebby claudiNo ratings yet
- (10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesDocument8 pages(10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesIsmail MuhammadNo ratings yet
- Anesthesia Regional y Sindrome Compartamental Nov 21Document5 pagesAnesthesia Regional y Sindrome Compartamental Nov 21ema moralesNo ratings yet
- 978 1 62808 567 9 - ch21Document13 pages978 1 62808 567 9 - ch21carrpahdfNo ratings yet
- Facial and Cochlear Nerve Complications Following Microsurgical Resection of Vestibular Schwannomas in A Series of 221 CasesDocument5 pagesFacial and Cochlear Nerve Complications Following Microsurgical Resection of Vestibular Schwannomas in A Series of 221 CasesSa'Deu FondjoNo ratings yet
- Alwahab2017 Article OccipitalMeningoencephaloceleC PDFDocument4 pagesAlwahab2017 Article OccipitalMeningoencephaloceleC PDFOvamelia JulioNo ratings yet
- Imaging of OrbitDocument69 pagesImaging of OrbitFaisal ShembeshNo ratings yet
- Peripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewDocument4 pagesPeripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Spinal Cord Injury RehabilitationDocument6 pagesSpinal Cord Injury RehabilitationHugh JacobsNo ratings yet
- Arachnoidal Diverticula of Sacral Extradural Meningeal CysDocument7 pagesArachnoidal Diverticula of Sacral Extradural Meningeal Cysjabarin.hNo ratings yet
- Surgical Management of Giant Intracranial Meningiomas: Original ArticleDocument6 pagesSurgical Management of Giant Intracranial Meningiomas: Original ArticleAdel SalehNo ratings yet
- Surgical Management of An Extensive Spinal EpiduraDocument5 pagesSurgical Management of An Extensive Spinal EpiduraqrscentralNo ratings yet
- AsianJNeurosurg102126-4310714 115827 PDFDocument3 pagesAsianJNeurosurg102126-4310714 115827 PDFSucipto HartonoNo ratings yet
- Transsphenoidal Hypophysectomy:: Postsurgical CT FindingsDocument6 pagesTranssphenoidal Hypophysectomy:: Postsurgical CT FindingsnurNo ratings yet
- Comparison of Two Approaches ofDocument96 pagesComparison of Two Approaches ofJacob OrtizNo ratings yet
- Minimally Invasive Posterior Cervical Foraminotomy: Microscopic Tubular Assisted (With Technical Tips)Document7 pagesMinimally Invasive Posterior Cervical Foraminotomy: Microscopic Tubular Assisted (With Technical Tips)Nasrullah nsrNo ratings yet
- Neurocysticercosis. A Frequent Cause of Seizures, Epilepsy, and OtherDocument12 pagesNeurocysticercosis. A Frequent Cause of Seizures, Epilepsy, and OtherMaria Lucero Jinés TapiaNo ratings yet
- Efficacy of Autologous Stem Cell Therapy in Femoral Head Avascular Necrosis: A Comparative StudyDocument7 pagesEfficacy of Autologous Stem Cell Therapy in Femoral Head Avascular Necrosis: A Comparative StudyApril RahmawatiNo ratings yet
- Legnani 2013Document6 pagesLegnani 2013wedawisnawaNo ratings yet
- Extended FBSDocument9 pagesExtended FBSlakshminivas PingaliNo ratings yet
- Thoracoscopic Sympathectomy Techniques and OutcomesDocument15 pagesThoracoscopic Sympathectomy Techniques and OutcomesBeshoy KhelaNo ratings yet
- Contralateral Approaches To Multiple Cerebral AneurysmsDocument4 pagesContralateral Approaches To Multiple Cerebral AneurysmsMorteza Mazloom Farsi BafNo ratings yet
- Evolution of The Surgical Management of Cauda Equina SyndromeDocument13 pagesEvolution of The Surgical Management of Cauda Equina SyndromeAtul JainNo ratings yet
- Neuro SurgeryDocument14 pagesNeuro Surgeryapi-3840195100% (4)
- Ko 2017Document14 pagesKo 2017Milton Ricardo de Medeiros FernandesNo ratings yet
- Aneurysmorrhaphy (Eng)Document14 pagesAneurysmorrhaphy (Eng)Harlan IdrisNo ratings yet
- Research ArticleDocument7 pagesResearch Articlefm_askaNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- Hydrocephalus With Lateral Ventricular Lesions Case Series and Review of LiteratureDocument10 pagesHydrocephalus With Lateral Ventricular Lesions Case Series and Review of Literaturemazen alkarrasNo ratings yet
- Extradural Anterior Clinoidectomy in Surgical Management of Clinoidal MeningiomasDocument11 pagesExtradural Anterior Clinoidectomy in Surgical Management of Clinoidal Meningiomasmazen alkarrasNo ratings yet
- The Inferior Nuchal Line As A Simple Landmark For Identifying The Vertebral Artery During The Retrosigmoid ApproachDocument7 pagesThe Inferior Nuchal Line As A Simple Landmark For Identifying The Vertebral Artery During The Retrosigmoid Approachmazen alkarrasNo ratings yet
- Assessment of The Outcome of Percutaneous Pedicle Screws in Management of Degenerative and Traumatic Dorsal and Lumbar PathologiesDocument8 pagesAssessment of The Outcome of Percutaneous Pedicle Screws in Management of Degenerative and Traumatic Dorsal and Lumbar Pathologiesmazen alkarrasNo ratings yet
- Bmjopen 2020 January 10 1 Inline Supplementary Material 1Document31 pagesBmjopen 2020 January 10 1 Inline Supplementary Material 1mazen alkarras100% (1)
- Bmjopen 2020 January 10 1 Inline Supplementary Material 1Document31 pagesBmjopen 2020 January 10 1 Inline Supplementary Material 1mazen alkarras100% (1)
- Bmjopen 2020 January 10 1 Inline Supplementary Material 1Document31 pagesBmjopen 2020 January 10 1 Inline Supplementary Material 1mazen alkarras100% (1)
- Ancient South Arabian TradeDocument16 pagesAncient South Arabian TradeAbo AliNo ratings yet
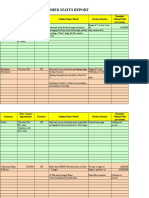
- Customer Status Update Report 27th January 2015 ColourDocument20 pagesCustomer Status Update Report 27th January 2015 ColourmaryNo ratings yet
- Sap GlossaryDocument324 pagesSap GlossaryNikos TataliasNo ratings yet
- GYROSCOPE ManualDocument8 pagesGYROSCOPE ManualAman BansalNo ratings yet
- Lesson 1 G8Document11 pagesLesson 1 G8Malorie Dela CruzNo ratings yet
- Congress Vienna QuestionsDocument5 pagesCongress Vienna QuestionsElliott CookNo ratings yet
- Hypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHDocument6 pagesHypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHLeyla SaabNo ratings yet
- Slings CatalogDocument152 pagesSlings CatalogtaNNertaroNo ratings yet
- Pharmaceutical and Software Development ProjectsDocument6 pagesPharmaceutical and Software Development ProjectsAlexandar123No ratings yet
- Importance of Plants in Our LivesDocument47 pagesImportance of Plants in Our LivesAlanie Grace Beron TrigoNo ratings yet
- Peter Linz An Introduction To Formal Languages and Automata Solution ManualDocument4 pagesPeter Linz An Introduction To Formal Languages and Automata Solution ManualEvelyn RM0% (2)
- Chapter 12 1Document15 pagesChapter 12 1Brigitte ReyesNo ratings yet
- Estudio ArminioDocument13 pagesEstudio ArminioJavier LópezNo ratings yet
- Herbivoría y Cristales de CaOxDocument33 pagesHerbivoría y Cristales de CaOxBrain LongwoodNo ratings yet
- L&T Type 2 Co-Ordination Selection ChartsDocument48 pagesL&T Type 2 Co-Ordination Selection Chartsrdeepak99100% (7)
- Tadano Hydraulic Rough Terrain Crane TR 350xl 3 560485 Operation Manual 1999 en JPDocument22 pagesTadano Hydraulic Rough Terrain Crane TR 350xl 3 560485 Operation Manual 1999 en JPmarcowens210992apd100% (126)
- Monitoring Rock and Soil Mass Performance: To The ConferenceDocument1 pageMonitoring Rock and Soil Mass Performance: To The ConferenceÉrica GuedesNo ratings yet
- Interconnection of Power SystemsDocument5 pagesInterconnection of Power SystemsRohan Sharma50% (2)
- Basic Encaustic Manual Author R&FDocument16 pagesBasic Encaustic Manual Author R&Fagustin arellanoNo ratings yet
- Inventions Crossword PuzzleDocument2 pagesInventions Crossword PuzzleAimri910% (1)
- Final CBLMDocument66 pagesFinal CBLMRanilyn UrbiztundoNo ratings yet
- Carco h90vsDocument9 pagesCarco h90vsRoxana Elizabeth Valencia NavarrteNo ratings yet
- Does Cash App Have Business Accounts - Google SeaDocument1 pageDoes Cash App Have Business Accounts - Google SeaAdedayo CrownNo ratings yet
- MAKING THINGS SIMPLER Review of Related LiteratureDocument72 pagesMAKING THINGS SIMPLER Review of Related Literaturejuju_batugal100% (1)
- CSCP Module 3Document10 pagesCSCP Module 3Asher50% (2)
- Mystic Mystique Face Reading-IIDocument10 pagesMystic Mystique Face Reading-IIVijay KumarNo ratings yet
- Lauren Tarshis - (I Survived 05) - I Survived The San Francisco Earthquake, 1906Document66 pagesLauren Tarshis - (I Survived 05) - I Survived The San Francisco Earthquake, 1906Olga de Ramos100% (1)