You might also like
- Power Gating - Power Management Technique: VLSI Basics and Interview QuestionsDocument12 pagesPower Gating - Power Management Technique: VLSI Basics and Interview QuestionsRohith RajNo ratings yet
- Air Transportation ReviewerDocument16 pagesAir Transportation ReviewerJuly BacarNo ratings yet
- 1 s2.0 S2212628721002589 MainDocument6 pages1 s2.0 S2212628721002589 MainEvans JohnNo ratings yet
- 1 s2.0 S2212628721000864 MainDocument5 pages1 s2.0 S2212628721000864 MainLuthfi LazuardiNo ratings yet
- Top Ten Pearls For Successful Hip ArthrosDocument10 pagesTop Ten Pearls For Successful Hip ArthrosMoustafa MohamedNo ratings yet
- Modifying Syme Amputation Prevents Heel Pad MigrationDocument5 pagesModifying Syme Amputation Prevents Heel Pad MigrationdamonenNo ratings yet
- Anterior Cruciate Ligament All InsideDocument7 pagesAnterior Cruciate Ligament All InsideVijay KumarNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- How To Avoid Varus Stem in THRDocument6 pagesHow To Avoid Varus Stem in THRPoliceNo ratings yet
- Anatomic Posterolateral Corner Reconstruction With AutograftsDocument7 pagesAnatomic Posterolateral Corner Reconstruction With AutograftsVõ Văn Phúc ToànNo ratings yet
- Cuadricepsplastia MipiDocument5 pagesCuadricepsplastia MipiVictor HernandezNo ratings yet
- Medicine The American Journal of SportsDocument8 pagesMedicine The American Journal of Sportshieuminhduong7No ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Cephalomedullary Nailing of Pertrochanteric Femur Fractures Using A Large Distractor and Standard Radiolucent TableDocument4 pagesCephalomedullary Nailing of Pertrochanteric Femur Fractures Using A Large Distractor and Standard Radiolucent Tabledrbane123No ratings yet
- Weller 2020Document10 pagesWeller 2020Deborah SalinasNo ratings yet
- MontotenniselbowDocument7 pagesMontotenniselbowPURVA THAKURNo ratings yet
- Total Elbow TechniqueDocument7 pagesTotal Elbow Techniquedidit satmokoNo ratings yet
- Early Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessDocument6 pagesEarly Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessJohannes CordeNo ratings yet
- Franci Oz I 2018Document7 pagesFranci Oz I 2018Carlos Mauricio Salazar BedollaNo ratings yet
- 1348 6456 4 PBDocument7 pages1348 6456 4 PB林良駿No ratings yet
- All-Epiphyseal, All-Inside Anterior Cruciate Ligament Reconstruction Technique For Skeletally Immature PatientsDocument9 pagesAll-Epiphyseal, All-Inside Anterior Cruciate Ligament Reconstruction Technique For Skeletally Immature Patientshieuminhduong7No ratings yet
- Autologous Tracheal Replacement Surgical Technique 2018 Thoracic Surgery CLDocument9 pagesAutologous Tracheal Replacement Surgical Technique 2018 Thoracic Surgery CLEdgar ForeroNo ratings yet
- Outside-In Capsulotomy of The Hip For Arthroscopic Pincer ResectionDocument6 pagesOutside-In Capsulotomy of The Hip For Arthroscopic Pincer ResectionMoustafa MohamedNo ratings yet
- Autologous Osteochondral Mosaicplasty For Osteochondritis Dissecans of The Elbow in Teenage AthletesDocument9 pagesAutologous Osteochondral Mosaicplasty For Osteochondritis Dissecans of The Elbow in Teenage AthletesAlejandro RamírezNo ratings yet
- Knupp 2011Document7 pagesKnupp 2011orlandoNo ratings yet
- Antegrade Intramedullary Screws in Metacarpal FracDocument6 pagesAntegrade Intramedullary Screws in Metacarpal FracLuis Guillermo Buitrago BuitragoNo ratings yet
- (Ii) Surgical Approaches To The Knee Joint: Anteromedial Parapatellar ApproachDocument8 pages(Ii) Surgical Approaches To The Knee Joint: Anteromedial Parapatellar ApproachDaniel G. A. C.No ratings yet
- Novel Surgical Technique For Clavicle Graft HarvestDocument5 pagesNovel Surgical Technique For Clavicle Graft Harvestsanchaita kohliNo ratings yet
- Subtrochanteric Osteotomy in Crowe IV Dysplastic HipsDocument7 pagesSubtrochanteric Osteotomy in Crowe IV Dysplastic HipsMohan DesaiNo ratings yet
- V1 PLCDocument18 pagesV1 PLCBartoszNo ratings yet
- Costochondral GraftsDocument5 pagesCostochondral Graftssmartdoc36100% (1)
- Columbus IQ InstrumentsDocument84 pagesColumbus IQ Instrumentst5cfdcw977No ratings yet
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- Autoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSDocument5 pagesAutoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSVillateAngelaNo ratings yet
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsDocument7 pagesTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersNo ratings yet
- Piis2212628719301896 PDFDocument7 pagesPiis2212628719301896 PDFIñigo Verdalet OlmedoNo ratings yet
- Analysis of Surgical Management of Proximal Humeral FracturesDocument5 pagesAnalysis of Surgical Management of Proximal Humeral FracturesRhizka djitmauNo ratings yet
- J ArthrnjknliDocument10 pagesJ ArthrnjknliJahid HasanNo ratings yet
- Pi Is 0363502317302241Document5 pagesPi Is 0363502317302241ashik MohamedNo ratings yet
- Does Use of A Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee ArthroplastyDocument6 pagesDoes Use of A Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee ArthroplastyAsmed El SalugNo ratings yet
- Devendra Et Al 2018 Vascular Injuries Due To Cerclage Passer Relevant Anatomy and Note of CautionDocument7 pagesDevendra Et Al 2018 Vascular Injuries Due To Cerclage Passer Relevant Anatomy and Note of CautionBruno HazlebyNo ratings yet
- Modified Stoppa Approach For Acetabular FixationDocument7 pagesModified Stoppa Approach For Acetabular FixationAthenaeum Scientific PublishersNo ratings yet
- Reconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyDocument9 pagesReconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyNorin FornaNo ratings yet
- Mandibular Surgery Technologic and Technical Improvements - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaDocument35 pagesMandibular Surgery Technologic and Technical Improvements - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaGabriela Lizbeth ArmentaNo ratings yet
- Osteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingDocument5 pagesOsteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingAnonymous Qt31LLO1lNo ratings yet
- Acromioclavicular Joint Dislocation: Repair Through Open Ligament Transfer and Nonabsorbable Suture FixationDocument8 pagesAcromioclavicular Joint Dislocation: Repair Through Open Ligament Transfer and Nonabsorbable Suture FixationParaliov TiberiuNo ratings yet
- Azar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureDocument4 pagesAzar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureKuozram No MasNo ratings yet
- Green 2013Document4 pagesGreen 2013Angel GutierrezNo ratings yet
- Multidirectional Instability of The Ankle: Surgical ReconstructionDocument7 pagesMultidirectional Instability of The Ankle: Surgical ReconstructionAnonymous kdBDppigENo ratings yet
- ACL Reconstruction Using Quadriceps Tendon: HE Utting DGEDocument5 pagesACL Reconstruction Using Quadriceps Tendon: HE Utting DGEDian FitriaNo ratings yet
- The Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegDocument7 pagesThe Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegMarco Antonio MiraveteNo ratings yet
- Introduction of A Guide Based On A Femoral Neck Se PDFDocument6 pagesIntroduction of A Guide Based On A Femoral Neck Se PDFStephenoNo ratings yet
- PCL AvulsionDocument4 pagesPCL Avulsionharpreet singhNo ratings yet
- Marcheggianimuccioli 2019Document12 pagesMarcheggianimuccioli 2019Ghusun MadaniNo ratings yet
- Upload Scribd 3Document5 pagesUpload Scribd 3Yoga AninditaNo ratings yet
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyDocument6 pagesSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebNo ratings yet
- Flexible 3D Laparoscopic Assisted Reduction andDocument9 pagesFlexible 3D Laparoscopic Assisted Reduction andgevowo3277No ratings yet
- AesculapDocument28 pagesAesculaplorenzocastaldiNo ratings yet
- Knee Disarticulation Versus Above-Knee Amputation : Balgrist Orthopaedic Hospital, University of ZurichDocument5 pagesKnee Disarticulation Versus Above-Knee Amputation : Balgrist Orthopaedic Hospital, University of ZurichAlfred JacksonNo ratings yet
- Lower Leg Reconstruction After Resection of A Squamous Cell CarcinomaDocument7 pagesLower Leg Reconstruction After Resection of A Squamous Cell CarcinomaOli BotaNo ratings yet
- Unicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsFrom EverandUnicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsTad L. GerlingerNo ratings yet
- Orthobullets CV QuestionsDocument127 pagesOrthobullets CV QuestionsNuno PaisNo ratings yet
- Injection-Based Management of Osteoarthritis of The Knee (SR of Guidelines 2021)Document6 pagesInjection-Based Management of Osteoarthritis of The Knee (SR of Guidelines 2021)Nuno PaisNo ratings yet
- AAOS Abstracts GuidelinesDocument6 pagesAAOS Abstracts GuidelinesNuno PaisNo ratings yet
- The 2020 NBA Orthobiologics Consensus Statement (2021)Document9 pagesThe 2020 NBA Orthobiologics Consensus Statement (2021)Nuno PaisNo ratings yet
- Krackow Stitch A Biomechanical Evaluation (2006)Document5 pagesKrackow Stitch A Biomechanical Evaluation (2006)Nuno PaisNo ratings yet
- Comparison of Joint Perception Between Posterior-Stabilized and Ultracongruent Total Knee Arthroplasty in The Same PatientDocument9 pagesComparison of Joint Perception Between Posterior-Stabilized and Ultracongruent Total Knee Arthroplasty in The Same PatientNuno PaisNo ratings yet
- AAOS Abstracts GuidelinesDocument2 pagesAAOS Abstracts GuidelinesNuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 20Document1 pageGamma3 Trochanteric Nail 180 Op Tech 20Nuno PaisNo ratings yet
- Gamma3 Nail Indications Precautions ContraindicationsDocument1 pageGamma3 Nail Indications Precautions ContraindicationsNuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 14Document1 pageGamma3 Trochanteric Nail 180 Op Tech 14Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 8Document1 pageGamma3 Trochanteric Nail 180 Op Tech 8Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 12Document1 pageGamma3 Trochanteric Nail 180 Op Tech 12Nuno PaisNo ratings yet
- Arthroscopic Meniscus Repair Rehab ProtocolDocument1 pageArthroscopic Meniscus Repair Rehab ProtocolNuno PaisNo ratings yet
- AAOS Abstracts GuidelinesDocument6 pagesAAOS Abstracts GuidelinesNuno PaisNo ratings yet
- Gamma3 Nail Design FeaturesDocument1 pageGamma3 Nail Design FeaturesNuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 17Document1 pageGamma3 Trochanteric Nail 180 Op Tech 17Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 6Document1 pageGamma3 Trochanteric Nail 180 Op Tech 6Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 4Document1 pageGamma3 Trochanteric Nail 180 Op Tech 4Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 2Document1 pageGamma3 Trochanteric Nail 180 Op Tech 2Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 7Document1 pageGamma3 Trochanteric Nail 180 Op Tech 7Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 3Document1 pageGamma3 Trochanteric Nail 180 Op Tech 3Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 56Document1 pageYamahaCS80-InstructionManual 56Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 44Document1 pageYamahaCS80-InstructionManual 44Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 41Document1 pageYamahaCS80-InstructionManual 41Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 42Document1 pageYamahaCS80-InstructionManual 42Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 38Document1 pageYamahaCS80-InstructionManual 38Nuno PaisNo ratings yet
- Gamma3 Trochanteric Nail 180 Op Tech 1Document1 pageGamma3 Trochanteric Nail 180 Op Tech 1Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 36Document1 pageYamahaCS80-InstructionManual 36Nuno PaisNo ratings yet
- YamahaCS80-InstructionManual 31Document1 pageYamahaCS80-InstructionManual 31Nuno PaisNo ratings yet
- Crimean-Congo Hemorrhagic Fever ReviewDocument31 pagesCrimean-Congo Hemorrhagic Fever ReviewfaizalNo ratings yet
- XFGRRRDocument100 pagesXFGRRRAbchoNo ratings yet
- Quality Testing of Honey StandardsDocument33 pagesQuality Testing of Honey StandardsK. N RaoNo ratings yet
- EVERBUILD® EVERFLEX® 565 Clean Room Silicone: Product Data SheetDocument3 pagesEVERBUILD® EVERFLEX® 565 Clean Room Silicone: Product Data Sheetsamira bashirvandNo ratings yet
- GeographyDocument18 pagesGeographyAshley Morgan88% (8)
- 38th Workshop On Geothermal PDFDocument25 pages38th Workshop On Geothermal PDFAulia KurniaNo ratings yet
- Analysis of Power Quality Issues and Implementation of UPQC Topologies To Enhance Power System StabilityDocument16 pagesAnalysis of Power Quality Issues and Implementation of UPQC Topologies To Enhance Power System StabilityEditor IJTSRDNo ratings yet
- Ce6101 Problem Sheet 3Document4 pagesCe6101 Problem Sheet 3HT BinhNo ratings yet
- Aberrant - Core BookDocument292 pagesAberrant - Core BookRodrigo Hky100% (7)
- Area and Circumference of CircleDocument17 pagesArea and Circumference of CircleJared VallesNo ratings yet
- Aero 12ADocument2 pagesAero 12AIrwin XavierNo ratings yet
- 3d Printing Thesis StatementDocument5 pages3d Printing Thesis Statementoabfziiig100% (2)
- Ensemble Marin OscillantDocument4 pagesEnsemble Marin OscillantRobson CarlosNo ratings yet
- Geometry QuotesDocument2 pagesGeometry Quotesalecksander2005No ratings yet
- Compact and Efficient: Rotary KilnsDocument4 pagesCompact and Efficient: Rotary KilnsNhaca100% (1)
- GNG1105 D Aut2013Document6 pagesGNG1105 D Aut2013oss6000No ratings yet
- Probability As A General Concept Can Be Defined As The Chance of An Event OccurDocument14 pagesProbability As A General Concept Can Be Defined As The Chance of An Event OccurMuhammad Adnan KhalidNo ratings yet
- Lukong Cornelius Fai - Feynman Path Integrals in Quantum Mechanics and Statistical Physics-CRC Press (2021)Document415 pagesLukong Cornelius Fai - Feynman Path Integrals in Quantum Mechanics and Statistical Physics-CRC Press (2021)Vi Kem100% (1)
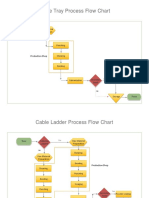
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- Vernacular ArchitectureDocument16 pagesVernacular ArchitectureHasita KrovvidiNo ratings yet
- HTTP Sleekfreak Ath CX 81 3wdev CD3WD METALWRK GTZ075CE B65 7 HTMDocument14 pagesHTTP Sleekfreak Ath CX 81 3wdev CD3WD METALWRK GTZ075CE B65 7 HTMPavan SripadaNo ratings yet
- Reservoir SedimentationDocument20 pagesReservoir SedimentationKathlienNo ratings yet
- Adobe Scan 11-Oct-2022Document5 pagesAdobe Scan 11-Oct-2022onkarkumarsolankiNo ratings yet
- The State of Madflya Pradesh: Chaptee SeconDocument38 pagesThe State of Madflya Pradesh: Chaptee Seconnavdeep tiwariNo ratings yet
- Aronne Armanini (Auth.) - Principles of River Hydraulics-Springer International Publishing (2018)Document230 pagesAronne Armanini (Auth.) - Principles of River Hydraulics-Springer International Publishing (2018)Matija LozicNo ratings yet
- VCTA-S810 OnlineDocument3 pagesVCTA-S810 OnlineqwUENo ratings yet
- Reflective EssayDocument5 pagesReflective Essaybwood17No ratings yet
- 986.33 Mesofilos Aerobios-PetrifilmDocument1 page986.33 Mesofilos Aerobios-PetrifilmBleidy NieblesNo ratings yet