You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Laboratory Tests and Diagnostic Procedures, 6E (2013) (UnitedVRG) PDFDocument1,235 pagesLaboratory Tests and Diagnostic Procedures, 6E (2013) (UnitedVRG) PDFrisovi100% (7)
- Urinary Physiology QDocument9 pagesUrinary Physiology QizabelaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
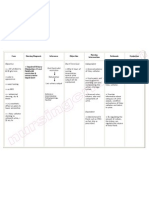
- Nursing Care Plan Impaired Urinary EliminationDocument1 pageNursing Care Plan Impaired Urinary Eliminationderic86% (14)
- Nursing Considerations For Routine UrinalysisDocument2 pagesNursing Considerations For Routine UrinalysisLord Pozak Miller0% (1)
- Chem41 Postlabexpt.n0.3Document36 pagesChem41 Postlabexpt.n0.3HJakansjakkaNo ratings yet
- Complementaria-Sternheimer-Malbin Staining To Detect Decoy Cells in Urine of 213Document6 pagesComplementaria-Sternheimer-Malbin Staining To Detect Decoy Cells in Urine of 213Roberto GutierrezNo ratings yet
- Platelet Transfusion Induces Alloimmunization To D and Non-D Rhesus AntigensDocument6 pagesPlatelet Transfusion Induces Alloimmunization To D and Non-D Rhesus AntigensRoberto GutierrezNo ratings yet
- Current Trends in Platelet Transfusions Practice - The Role of ABO-RhD and Human Leukocyte Antigen IncompatibilityDocument13 pagesCurrent Trends in Platelet Transfusions Practice - The Role of ABO-RhD and Human Leukocyte Antigen IncompatibilityRoberto GutierrezNo ratings yet
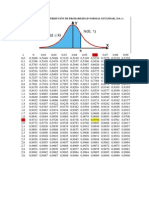
- Áreas Bajo La Distribución de Probabilidad Normal Estándar, N (0, 1)Document1 pageÁreas Bajo La Distribución de Probabilidad Normal Estándar, N (0, 1)Roberto GutierrezNo ratings yet
- UrinalysisDocument77 pagesUrinalysisAudreyNo ratings yet
- Stone BreakerDocument10 pagesStone BreakerrkmkbkNo ratings yet
- Kidney Stones - Symptoms, Causes, Types, and Treatment - National Kidney FoundationDocument11 pagesKidney Stones - Symptoms, Causes, Types, and Treatment - National Kidney FoundationamanuelNo ratings yet
- 24-Urine Collection - NsoDocument3 pages24-Urine Collection - NsojamesNo ratings yet
- The Joy of Eating-The Alkaline WayDocument60 pagesThe Joy of Eating-The Alkaline WayFrank Pluta100% (3)
- 30-20-DX-489-76 Atellica Menu US FINALDocument2 pages30-20-DX-489-76 Atellica Menu US FINALoctavio omar villegasNo ratings yet
- Urinalysis Presentation1Document25 pagesUrinalysis Presentation1OliviaLaneNo ratings yet
- Assessment of Renal and Urinary Tract FunctionDocument19 pagesAssessment of Renal and Urinary Tract FunctionokaciaNo ratings yet
- Diabetes Chart.1Document6 pagesDiabetes Chart.1dr_vidyasagar41No ratings yet
- Aubf 2Document2 pagesAubf 2Gerald John PazNo ratings yet
- Urinalysis PDFDocument56 pagesUrinalysis PDFTio AjhaNo ratings yet
- RosellaDocument7 pagesRosellaGaluh WulanNo ratings yet
- ICSE Solutions For Class 10 Biology - The Excretory System - A Plus TopperDocument28 pagesICSE Solutions For Class 10 Biology - The Excretory System - A Plus TopperSuresh Kumar100% (1)
- Prinsip Pemeriksaan Urin Rutin - 1Document6 pagesPrinsip Pemeriksaan Urin Rutin - 1AdnanNo ratings yet
- Infinity Urea Liquid Reagent ENDocument2 pagesInfinity Urea Liquid Reagent ENKouame FrancisNo ratings yet
- Complete Guide To Urine TheraphyDocument9 pagesComplete Guide To Urine TheraphyNancy Miro100% (4)
- Activity and ExerciseDocument30 pagesActivity and ExerciseSIVA KRISHNA PRASAD ARJANo ratings yet
- Organs in The Excretory System and Their Functions (4) - Poonam SinghDocument6 pagesOrgans in The Excretory System and Their Functions (4) - Poonam SinghDazelyn OsiasNo ratings yet
- NCP Urinary Tract InfectionDocument4 pagesNCP Urinary Tract InfectiondollythesheepNo ratings yet
- Bayombong, Nueva Vizcaya 3700 Nursing DepartmentDocument9 pagesBayombong, Nueva Vizcaya 3700 Nursing DepartmentKyla CarbonelNo ratings yet
- UrinalysisDocument5 pagesUrinalysisKreshnik HAJDARINo ratings yet
- Excretory System PresentationDocument12 pagesExcretory System Presentationapi-263389150No ratings yet
- Urine Therapy For Any Kind of DiseasesDocument6 pagesUrine Therapy For Any Kind of DiseasesVipula Parekh60% (5)
- Lecture 2 - Urine ExaminationDocument62 pagesLecture 2 - Urine ExaminationmihalachemirelaNo ratings yet
- Nursing Manual OptDocument151 pagesNursing Manual OptNjoku StephenNo ratings yet