You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Making The GradeDocument4 pagesMaking The Gradejuancho1994No ratings yet
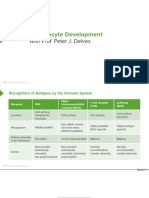
- 18 Slides Recognition of Antigens Lymphocyte DevelopmentDocument3 pages18 Slides Recognition of Antigens Lymphocyte Developmentjuancho1994No ratings yet
- Constructores de Paz1Document4 pagesConstructores de Paz1juancho1994No ratings yet
- 18 Slides Recognition of Antigens Lymphocyte DevelopmentDocument3 pages18 Slides Recognition of Antigens Lymphocyte Developmentjuancho1994No ratings yet
- Questionnaire SMDocument8 pagesQuestionnaire SMTina chackoNo ratings yet
- Complex OdontomasDocument1 pageComplex OdontomasAnkita AroraNo ratings yet
- AHFS Drug InformationDocument10 pagesAHFS Drug InformationMika FebryatiNo ratings yet
- The Anatomy of The Coronary SinusDocument7 pagesThe Anatomy of The Coronary Sinusmihalcea alinNo ratings yet
- HS202 Pathology ExamDocument6 pagesHS202 Pathology ExamJulio dR AltavasNo ratings yet
- Biologia PlantelorDocument23 pagesBiologia PlantelorCristina Teodora BerbecaruNo ratings yet
- An Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFkatherine dayagNo ratings yet
- Liver CancerDocument233 pagesLiver CancerandikhgNo ratings yet
- Substance Abuse TutorialsDocument3 pagesSubstance Abuse TutorialsjasmingabrielNo ratings yet
- Beyond Medicalisation - N. RoseDocument3 pagesBeyond Medicalisation - N. RoseManuel Guerrero Antequera100% (1)
- Laporan Supernova Wiji - AgustusDocument5 pagesLaporan Supernova Wiji - Agustusrahma dewi styaningrumNo ratings yet
- Learning Plan Semester 3Document3 pagesLearning Plan Semester 3api-314566363100% (1)
- WorldCPDayCP InfographicDocument1 pageWorldCPDayCP InfographicquietfoolNo ratings yet
- PMLS 2 Compilation Notes 2Document77 pagesPMLS 2 Compilation Notes 2seaynNo ratings yet
- Seminar TopicsDocument4 pagesSeminar TopicsVimal NishadNo ratings yet
- Instruments: 1. Vim Silver Man'S Biopsy Needle For Liver Biopsy Two MethodsDocument11 pagesInstruments: 1. Vim Silver Man'S Biopsy Needle For Liver Biopsy Two Methodstasneem faizaNo ratings yet
- Styles of Acupuncture in Current Practice - Martin WangDocument104 pagesStyles of Acupuncture in Current Practice - Martin WangТом Вейцман100% (1)
- NCM 107 Maternal and Child Nursing Related Learning Experience BSN 2 AY 2020-2021Document18 pagesNCM 107 Maternal and Child Nursing Related Learning Experience BSN 2 AY 2020-2021janina myka100% (1)
- Risk-For-Infection Sample NCPDocument3 pagesRisk-For-Infection Sample NCPDuane Liloc0% (1)
- Final Project RubricDocument3 pagesFinal Project Rubricapi-436796283No ratings yet
- X Ray UwuDocument15 pagesX Ray UwuTulika BholaNo ratings yet
- Drug StudyDocument3 pagesDrug StudyTacuyan AlphaNo ratings yet
- IpcrDocument4 pagesIpcrEdrheyl Limbaga BiadnesNo ratings yet
- SIF Determination & CategorizationDocument1 pageSIF Determination & CategorizationJosé ArévalosNo ratings yet
- Diagnosis Hepatitis PDFDocument18 pagesDiagnosis Hepatitis PDFYuendri IrawantoNo ratings yet
- McqsDocument3 pagesMcqsadham bani younesNo ratings yet
- Hydrogen Peroxide Cancer TreatmentDocument25 pagesHydrogen Peroxide Cancer TreatmentLoreen100% (2)
- Brain TumorDocument1 pageBrain TumorChase XerolfNo ratings yet
- Patient-Centred CareDocument15 pagesPatient-Centred CareMwanja MosesNo ratings yet
- A Follow Up Study of Early Treatment of Pseudo Class III MalocclusionDocument8 pagesA Follow Up Study of Early Treatment of Pseudo Class III MalocclusionL Andrea CardenasNo ratings yet