You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Food and NutritionDocument36 pagesFood and NutritionM.g. Alomia67% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
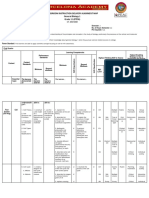
- Classroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)Document6 pagesClassroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)JunedelMirallesPerez50% (2)
- Feeding PDF Feeding History QuesDocument8 pagesFeeding PDF Feeding History QuesSophia DaniilNo ratings yet
- Hyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMODocument63 pagesHyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMOAkbar AmirullahNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Visa Appointment of LetterDocument3 pagesVisa Appointment of LetterRaaz SharmaNo ratings yet
- New Biophilia FeaturesDocument14 pagesNew Biophilia Featuresdues babaoNo ratings yet
- Design StudyDocument9 pagesDesign StudySylvia DamayantiNo ratings yet
- Dance Intervention Effects On Physical Function in Healthy Older Adults: A Systematic Review and Meta AnalysisDocument11 pagesDance Intervention Effects On Physical Function in Healthy Older Adults: A Systematic Review and Meta AnalysisSylvia DamayantiNo ratings yet
- Parkinsonism and Related Disorders: M.J. de Dreu, A.S.D. Van Der Wilk, E. Poppe, G. Kwakkel, E.E.H. Van WegenDocument6 pagesParkinsonism and Related Disorders: M.J. de Dreu, A.S.D. Van Der Wilk, E. Poppe, G. Kwakkel, E.E.H. Van WegenSylvia DamayantiNo ratings yet
- Jurnal TunggalDocument9 pagesJurnal TunggalSylvia DamayantiNo ratings yet
- Intervensi DomainDocument92 pagesIntervensi DomainSylvia DamayantiNo ratings yet
- Immobilization in External RotationDocument9 pagesImmobilization in External RotationSylvia DamayantiNo ratings yet
- Cardiac SurgeryDocument10 pagesCardiac SurgerySylvia DamayantiNo ratings yet
- Hamstring Injury Prevention in Belgian and English Elite Football TeamsDocument8 pagesHamstring Injury Prevention in Belgian and English Elite Football TeamsSylvia DamayantiNo ratings yet
- A Study in Group Therapy For Veterans With PTSDDocument7 pagesA Study in Group Therapy For Veterans With PTSDJack FreedmanNo ratings yet
- Characteristic of Selected Soil Streptomycetes With Antimicrobial Potential Against Phytopathogenic MicroorganismsDocument21 pagesCharacteristic of Selected Soil Streptomycetes With Antimicrobial Potential Against Phytopathogenic Microorganismsvijayrasigan786No ratings yet
- Gene Therapy: Laguna State Polytechnic University San Pablo CityDocument11 pagesGene Therapy: Laguna State Polytechnic University San Pablo CityAndromeda GalaxyNo ratings yet
- POI Lab ReviewerDocument2 pagesPOI Lab ReviewerJerick JusayNo ratings yet
- Is Stress Good For YouDocument3 pagesIs Stress Good For YoupavankumarmtNo ratings yet
- MicrosatellitesDocument24 pagesMicrosatellitesAhmed BioNo ratings yet
- Dengue Fever With Uti: To: DR - Swathi From: D.Vamshi Krishna Roll No: 15CE1T0024Document20 pagesDengue Fever With Uti: To: DR - Swathi From: D.Vamshi Krishna Roll No: 15CE1T0024surineni manishaNo ratings yet
- Beans and Other Legumes - Types and Cooking TipsDocument6 pagesBeans and Other Legumes - Types and Cooking TipsDisha TNo ratings yet
- Journal EntryDocument2 pagesJournal EntryABDULJAMIR GAYAKNo ratings yet
- Fresh Air Camp Application 2010Document13 pagesFresh Air Camp Application 2010Morgan Memorial Goodwill IndustriesNo ratings yet
- Tourism Leaflets: Where You Will Feel Exclusive and UniqueDocument2 pagesTourism Leaflets: Where You Will Feel Exclusive and UniqueNiveetha GunendranNo ratings yet
- Decompression SurgeryDocument9 pagesDecompression Surgeryapi-238049665No ratings yet
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- 800 Tavill Anatomy-Physiology-Liver PDFDocument29 pages800 Tavill Anatomy-Physiology-Liver PDFSheen AponNo ratings yet
- Septic Shock: Ask The ExpertDocument4 pagesSeptic Shock: Ask The ExpertIvy Dianne PascualNo ratings yet
- Nephrotic Syndrome (Nephrosis)Document9 pagesNephrotic Syndrome (Nephrosis)Madhusmita SatapathyNo ratings yet
- Clinphar M2-M3 Answer Case StudyDocument1 pageClinphar M2-M3 Answer Case StudyGwen Myles JoverNo ratings yet
- Water Pollution TP b38Document12 pagesWater Pollution TP b38Aaditya Pandey AmritNo ratings yet
- A Study On Traditional Mother Care PlantsDocument6 pagesA Study On Traditional Mother Care PlantsBarnali DuttaNo ratings yet
- 51 Ways To Fight Hay Fever and Other AllergiesDocument17 pages51 Ways To Fight Hay Fever and Other AllergiesvalentinNo ratings yet
- RFID Chip will Poison Me and Kill me if I Disobey. Microchip Implants - RFID Brain Chip : Crime, Malpratice, Mindcontrol, Sexual Abuse, Brain Abuse, Torture Abuse, Medical Abuse, and The Silent Killers via RFID Brain ChipDocument3 pagesRFID Chip will Poison Me and Kill me if I Disobey. Microchip Implants - RFID Brain Chip : Crime, Malpratice, Mindcontrol, Sexual Abuse, Brain Abuse, Torture Abuse, Medical Abuse, and The Silent Killers via RFID Brain ChipJohanNo ratings yet
- Furcation Involvement Classification - A Literature ReviewDocument6 pagesFurcation Involvement Classification - A Literature Reviewsasi dharanNo ratings yet
- COVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateDocument86 pagesCOVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateXochilt Mejia GarciaNo ratings yet