You might also like
- Admission Open For MPhil, MS, MSC 2022Document1 pageAdmission Open For MPhil, MS, MSC 2022Mazhar AliNo ratings yet
- Admissions Open For MphilDocument1 pageAdmissions Open For MphilMazhar AliNo ratings yet
- Certificate / Degree Board / University Passing Year Total Marks / GPA Obtained Marks / GPADocument1 pageCertificate / Degree Board / University Passing Year Total Marks / GPA Obtained Marks / GPAMazhar AliNo ratings yet
- Introduction To Computing (CS101) : Assignment # 01 Spring 2021Document4 pagesIntroduction To Computing (CS101) : Assignment # 01 Spring 2021Mazhar AliNo ratings yet
- Flood Bulletin BDocument1 pageFlood Bulletin BMazhar AliNo ratings yet
- Piwi 4Document15 pagesPiwi 4Mazhar AliNo ratings yet
- Fee Remission Form For OrphansDocument1 pageFee Remission Form For OrphansMazhar AliNo ratings yet
- Course Title: DNA Techniques and Clinical Application Course Code: BCHM-33104 Credit Hours: 3Document29 pagesCourse Title: DNA Techniques and Clinical Application Course Code: BCHM-33104 Credit Hours: 3Mazhar AliNo ratings yet
- Vince Buonaccorsi Associate Professor of Biology Juniata CollegeDocument76 pagesVince Buonaccorsi Associate Professor of Biology Juniata CollegeMazhar AliNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- RAPID AST FROM BLOOD CULUTURE-Methodology - EUCAST - RAST - v1 - 20181126 PDFDocument3 pagesRAPID AST FROM BLOOD CULUTURE-Methodology - EUCAST - RAST - v1 - 20181126 PDFKhoa Vi Sinh BVCRNo ratings yet
- Fact Sheet: Vancomycin-Resistant Enterococci (VRE)Document3 pagesFact Sheet: Vancomycin-Resistant Enterococci (VRE)roroanjniiNo ratings yet
- The Genera of Lactic Acid Bacteria - Wood (1995)Document414 pagesThe Genera of Lactic Acid Bacteria - Wood (1995)ISRAELNo ratings yet
- Med AtbDocument3 pagesMed AtbพัชรพลนะเออNo ratings yet
- Vancomycin Resistant EnterococciDocument238 pagesVancomycin Resistant EnterococciNoha Alaa EldinNo ratings yet
- Istoric: Din Antichitate Pina in Sec. 19Document303 pagesIstoric: Din Antichitate Pina in Sec. 19Lyly LylyNo ratings yet
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Document12 pagesIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNo ratings yet
- A Study On The Bacteriological Profile of Urinary PDFDocument4 pagesA Study On The Bacteriological Profile of Urinary PDFcendy oktariNo ratings yet
- Manual, Bacteria and Yeast Work UpDocument12 pagesManual, Bacteria and Yeast Work UpFilipus HendiantoNo ratings yet
- Peritonitis Update On Pathophysiology, Clinical Manifestations, and PDFDocument11 pagesPeritonitis Update On Pathophysiology, Clinical Manifestations, and PDFAnonymous InJS6aYZ100% (1)
- Lactic Acid Bacteria Fundamentals and Practice PDFDocument536 pagesLactic Acid Bacteria Fundamentals and Practice PDFIrving Mayo100% (3)
- Biochemical Test For Enterococcus SPDocument6 pagesBiochemical Test For Enterococcus SPganbio1981No ratings yet
- Peritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementDocument11 pagesPeritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementMuhamad Chairul SyahNo ratings yet
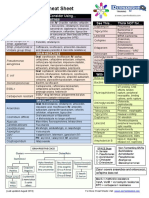
- Antibiotic Study Cheat Sheet August 2019Document1 pageAntibiotic Study Cheat Sheet August 2019Ryan TurnerNo ratings yet
- Azide Dextrose BrothDocument1 pageAzide Dextrose BrothJHOSELINE KHATERINE RAMIREZ BARBARANNo ratings yet
- The Rise of Enterococcus Beyond Vancomycin ResistanceDocument26 pagesThe Rise of Enterococcus Beyond Vancomycin ResistanceAPC consultoriaNo ratings yet
- MicrobiologyDocument81 pagesMicrobiologyAmanuel MaruNo ratings yet
- Food MicrobiologyDocument7 pagesFood MicrobiologyJuan Jose Escobar P.No ratings yet
- New Jersey Health Department Report RE: Dr. John VecchioneDocument11 pagesNew Jersey Health Department Report RE: Dr. John VecchioneNews12NJWebNo ratings yet
- Streptococcus and EnterococcusDocument91 pagesStreptococcus and EnterococcusAllyah Ross DuqueNo ratings yet
- Infectious Diseases of The Female Genital TractDocument1,111 pagesInfectious Diseases of The Female Genital TractJohn Ntokos100% (2)
- Biological and Physicochemical Indicators of Water Quality in Libreville and Its SurroundingsDocument7 pagesBiological and Physicochemical Indicators of Water Quality in Libreville and Its SurroundingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 - Systemic BacteriologyDocument316 pages1 - Systemic BacteriologyAlsirNo ratings yet
- Research Proposal CapsuleDocument12 pagesResearch Proposal CapsuleClaire GonoNo ratings yet
- A Seminar On Microgansims of Public Health Importance in WaterDocument40 pagesA Seminar On Microgansims of Public Health Importance in Waterjoe topeNo ratings yet
- Reference: 01-592 Technical Data Sheet Product: Bile Esculin Azide AgarDocument2 pagesReference: 01-592 Technical Data Sheet Product: Bile Esculin Azide AgarGeoemilia1No ratings yet
- List of Available Analysis 2022Document10 pagesList of Available Analysis 2022oubaha happyNo ratings yet
- Daptomycin 5Document2 pagesDaptomycin 5SachithNo ratings yet
- Chapter 22 Streptococcus, Enterococcus and PneumococcusDocument73 pagesChapter 22 Streptococcus, Enterococcus and PneumococcusPriyanshiNo ratings yet
- Clinical Efficacy of Fosfomycin For The Treatment of Complicated Lower Tract and Uncomplicated Urinary Tract InfectionsDocument7 pagesClinical Efficacy of Fosfomycin For The Treatment of Complicated Lower Tract and Uncomplicated Urinary Tract InfectionsInternational Medical PublisherNo ratings yet