You might also like
- Assignment/ Tugasan - Nursing Health AssessmentDocument8 pagesAssignment/ Tugasan - Nursing Health AssessmentSYafikFikkNo ratings yet
- Inborn Errors or MetabolismDocument25 pagesInborn Errors or MetabolismSamdiSutantoNo ratings yet
- Prep 2015Document358 pagesPrep 2015a alrabiaahNo ratings yet
- Case Study On Head InjuryDocument58 pagesCase Study On Head InjuryISLAMIC KNOWLEDGE BASED ON TRULY HADIS50% (2)
- Hematinics BPTDocument17 pagesHematinics BPTbpt2No ratings yet
- Nutrition and Metabolism: Vitamins Presented Dr. Alhaji GblaDocument23 pagesNutrition and Metabolism: Vitamins Presented Dr. Alhaji GblaAlhaji GblaNo ratings yet
- Anti Anemic DrugsDocument31 pagesAnti Anemic DrugsAmanda Samurti Pertiwi100% (1)
- What Are Trace Elements?: - Their Deficiency and Excess StatesDocument8 pagesWhat Are Trace Elements?: - Their Deficiency and Excess StatesRifdahavivahNo ratings yet
- VitaminsDocument32 pagesVitaminsdivya100% (5)
- Drug-Induced Nutrient DepletionDocument75 pagesDrug-Induced Nutrient DepletionValentin Quinteros100% (1)
- Inborn Errors of MetabolismDocument61 pagesInborn Errors of MetabolismVinay PatilNo ratings yet
- Nutritional Aspects of Urogenital DiseasesDocument80 pagesNutritional Aspects of Urogenital DiseasesAmirah Jihan AfryNo ratings yet
- VitaminsDocument37 pagesVitaminsMaryNo ratings yet
- Vitamin StudentDocument63 pagesVitamin StudenttienesemNo ratings yet
- IEM ScreeningDocument68 pagesIEM ScreeningKota AnuroopNo ratings yet
- Vitamins TableDocument1 pageVitamins TableMicah Lou CalambaNo ratings yet
- Haematinic Deficiencies (Iron, Vit B12 and Folate)Document7 pagesHaematinic Deficiencies (Iron, Vit B12 and Folate)Francesca Li100% (1)
- Inborn Errors of Metabolism Student LectureDocument81 pagesInborn Errors of Metabolism Student LectureFavourNo ratings yet
- Pharmacology: Andrea Q. Carigma, R.PH., M.D. May 2015Document46 pagesPharmacology: Andrea Q. Carigma, R.PH., M.D. May 2015Leonibel GhloeNo ratings yet
- سموم نظري٣Document6 pagesسموم نظري٣مصطفى ابراهيم سعيدNo ratings yet
- Vitamin and Trace Mineral Deficiency and ExcessDocument10 pagesVitamin and Trace Mineral Deficiency and ExcessenyowNo ratings yet
- CH 32 - Bone Mineral HomeostasisDocument4 pagesCH 32 - Bone Mineral HomeostasisNiki NourNo ratings yet
- Lecture 22. Drugs Used in Renal and Urinary Tract DisordersDocument38 pagesLecture 22. Drugs Used in Renal and Urinary Tract DisorderskrisnadewirahadiNo ratings yet
- Inborn Errors of Amino Acid MetabolismDocument65 pagesInborn Errors of Amino Acid MetabolismSantino MajokNo ratings yet
- Disorders of The BoneDocument2 pagesDisorders of The BoneRPh Krishna Chandra JagritNo ratings yet
- Mitochondrial DiseasesDocument34 pagesMitochondrial DiseasesAli MansorNo ratings yet
- Parathyroid Agents PDFDocument32 pagesParathyroid Agents PDFRhodee Kristine DoñaNo ratings yet
- Parathyroid Agents PDFDocument32 pagesParathyroid Agents PDFRhodee Kristine DoñaNo ratings yet
- MetaScreen 100+ Conditions DeckDocument115 pagesMetaScreen 100+ Conditions DeckLab Brawijaya HospitalNo ratings yet
- Class: Calcium Salts: Agent(s) Common Uses Contraindications Route/Dosage Onset of Action InteractionsDocument8 pagesClass: Calcium Salts: Agent(s) Common Uses Contraindications Route/Dosage Onset of Action InteractionsAlano S. LimgasNo ratings yet
- TABLE 17-24 - Some Causes of HypocalcemiaDocument1 pageTABLE 17-24 - Some Causes of HypocalcemiaRashmeeta ThadhaniNo ratings yet
- Inborn Errors of Metabolismiem Lecture 1Document32 pagesInborn Errors of Metabolismiem Lecture 1EMMANUEL ABEL IMAH100% (1)
- Vitamins and MineralsDocument91 pagesVitamins and MineralsPyaesone AungNo ratings yet
- Amino Acids Metabolism-Disorders-1Document19 pagesAmino Acids Metabolism-Disorders-1lucky mbaselaNo ratings yet
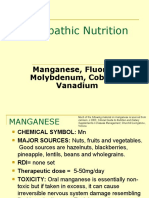
- Naturopathic Nutrition: Manganese, Fluoride, Molybdenum, Cobalt & VanadiumDocument16 pagesNaturopathic Nutrition: Manganese, Fluoride, Molybdenum, Cobalt & Vanadiumglenn johnstonNo ratings yet
- 1.3 Macrocytic Anaemia, Megaloblastic and Nonmegaloblastic AnaemiaDocument43 pages1.3 Macrocytic Anaemia, Megaloblastic and Nonmegaloblastic AnaemiaAlex KamougerosNo ratings yet
- Pharmacards CompilationDocument53 pagesPharmacards CompilationchristianfcualNo ratings yet
- Anti-Anemic Drugs - 210619200800Document40 pagesAnti-Anemic Drugs - 210619200800Yohannes MeridNo ratings yet
- Osteomalacia Ni Bro 1Document13 pagesOsteomalacia Ni Bro 1Brittany Lei MaquirayaNo ratings yet
- Vitamin D DeficiencyDocument11 pagesVitamin D DeficiencyElvisNo ratings yet
- AnemiaDocument26 pagesAnemiaIrtiza ChohanNo ratings yet
- Rickets in ChildrenDocument61 pagesRickets in ChildrenmdNo ratings yet
- Amino Acids Metabolism-DisordersDocument19 pagesAmino Acids Metabolism-Disorderslucky mbaselaNo ratings yet
- Drug Induced Liver InjuryDocument21 pagesDrug Induced Liver Injurytata ciripahNo ratings yet
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocument21 pagesDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Basic Need For GeriatricsDocument38 pagesBasic Need For GeriatricsMuhammad Yatsrib SemmeNo ratings yet
- Agussalim Bukhari Department of Nutrition Faculty of Medicine, Hasanuddin UniversityDocument37 pagesAgussalim Bukhari Department of Nutrition Faculty of Medicine, Hasanuddin Universitynini100% (1)
- Folate Metabolism and Macrocytic Anaemia: by DR (MRS) Baulch E.KDocument49 pagesFolate Metabolism and Macrocytic Anaemia: by DR (MRS) Baulch E.KPrincewill SeiyefaNo ratings yet
- Naturopathic Nutrition: Trace Elements: Zinc, Copper, Chromium, Boron & SeleniumDocument38 pagesNaturopathic Nutrition: Trace Elements: Zinc, Copper, Chromium, Boron & Seleniumglenn johnstonNo ratings yet
- Drug Study:: Name: Maria Chrislyn M. Genorga Yr - Sec: BSN 2ADocument2 pagesDrug Study:: Name: Maria Chrislyn M. Genorga Yr - Sec: BSN 2AVic Intia PaaNo ratings yet
- Unit 06: Drugs Acting On The Gastrointestinal SystemDocument9 pagesUnit 06: Drugs Acting On The Gastrointestinal SystemDental LecturesMMQNo ratings yet
- Hypocalcemia: Dept of Nephrology PsriDocument40 pagesHypocalcemia: Dept of Nephrology Psriind78No ratings yet
- Nutritional Management On Kidney Disease: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK 2018Document108 pagesNutritional Management On Kidney Disease: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK 2018Rahmawati HamudiNo ratings yet
- Renal Disease of Small AnimalsDocument46 pagesRenal Disease of Small AnimalsTahir KasimNo ratings yet
- Bio NotesDocument24 pagesBio NotesIslam MansourNo ratings yet
- Vit DEKDocument45 pagesVit DEKainslienNo ratings yet
- Vitamin Mineral Reference GuideDocument2 pagesVitamin Mineral Reference GuideEleni KostaraNo ratings yet
- AnemiaDocument40 pagesAnemiaGreenNo ratings yet
- DIABETESDocument43 pagesDIABETESY. Beatrice AbigailNo ratings yet
- Dietary Vitamins: Agussalim Bukhari Department of Nutrition Faculty of Medicine, Hasanuddin UniversityDocument37 pagesDietary Vitamins: Agussalim Bukhari Department of Nutrition Faculty of Medicine, Hasanuddin UniversityNurul fatimahNo ratings yet
- First Aid For The Usmle Step 1 2022-Mcgraw-Hill Education 2022Document1 pageFirst Aid For The Usmle Step 1 2022-Mcgraw-Hill Education 2022Beto RendonNo ratings yet
- Drug InteractionDocument1 pageDrug InteractionChrissieNo ratings yet
- CHN 104Document1 pageCHN 104May MayNo ratings yet
- NSC QuizDocument167 pagesNSC QuizTalal MehfoozNo ratings yet
- Ivermectin (Systemic) - Pediatric Drug Information - UpToDateDocument23 pagesIvermectin (Systemic) - Pediatric Drug Information - UpToDateFrank Harry LampardNo ratings yet
- Tuberculosis: GlobalDocument75 pagesTuberculosis: GlobalNAILA NEVES DE JESUSNo ratings yet
- Massage - The Scientific Basis of An Ancient Art Part 1 The Technics PDFDocument4 pagesMassage - The Scientific Basis of An Ancient Art Part 1 The Technics PDFMiki ShimizuNo ratings yet
- Halima Bf2Document30 pagesHalima Bf2halima alzadjaliNo ratings yet
- Oseltamivir (Tamifluw) and Its Potential For UseDocument17 pagesOseltamivir (Tamifluw) and Its Potential For UseRafael MusicasNo ratings yet
- A Case Study OnDocument176 pagesA Case Study OnTasneem MamokanNo ratings yet
- Test I. Identification Directions: Read The Statements Carefully and Put A Check ( ) Mark If The Statement Is An OpinionDocument2 pagesTest I. Identification Directions: Read The Statements Carefully and Put A Check ( ) Mark If The Statement Is An OpinionJundell DiazNo ratings yet
- Fixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFDocument6 pagesFixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFJejeNo ratings yet
- Zhineng Articles & ExercisesDocument41 pagesZhineng Articles & Exercisesdqtstock9555100% (1)
- WOD12 ReportDocument28 pagesWOD12 ReportDan MihailescuNo ratings yet
- Cultural Formulation Interview Final ManuscriptDocument38 pagesCultural Formulation Interview Final ManuscriptAnanta ChaliseNo ratings yet
- Concomitant SquintDocument21 pagesConcomitant SquintShivani Nair100% (1)
- Ngày thi: 11/6/2021 Thời gian làm bài: 60 phút, không kể thời gian phát đề Đề Thi Chính Thức (Đề có 5 trang)Document5 pagesNgày thi: 11/6/2021 Thời gian làm bài: 60 phút, không kể thời gian phát đề Đề Thi Chính Thức (Đề có 5 trang)Phi VyNo ratings yet
- Hypothermia Prevention - Survial in Cold Water - Minnesota Sea GrantDocument12 pagesHypothermia Prevention - Survial in Cold Water - Minnesota Sea GrantMarius SahajNo ratings yet
- Immunisation Schedule Victoria-November 2021Document6 pagesImmunisation Schedule Victoria-November 2021Julie PanditNo ratings yet
- Fluids, Electrolytes, Acid-Base Disorders, and Nutrition SupportDocument56 pagesFluids, Electrolytes, Acid-Base Disorders, and Nutrition SupportFarryrazaNo ratings yet
- New New EFT - Doc Only)Document46 pagesNew New EFT - Doc Only)rav007100% (4)
- Anti BacDocument4 pagesAnti BacCarolina RinconNo ratings yet
- Musculoskeletal System - Congenital AbnormalitiesDocument49 pagesMusculoskeletal System - Congenital AbnormalitiesShafiq Mohd Nor100% (1)
- PollutionDocument32 pagesPollutionPraveen Gaur67% (3)
- Evaluation of Male Partner Participation in Prevention of Mother To Child Transmission of HIVAIDs at Hoima Referral HospitalDocument14 pagesEvaluation of Male Partner Participation in Prevention of Mother To Child Transmission of HIVAIDs at Hoima Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Menstrual Blood BankingDocument60 pagesMenstrual Blood BankingMounika Bhallam100% (1)
- Health Administration at The Centre and State LevelDocument22 pagesHealth Administration at The Centre and State Levelmerin sunil100% (1)
- Prostate Acinar Adenocarcinoma Gleason Grading: Often Disqualifies From Active SurveillanceDocument2 pagesProstate Acinar Adenocarcinoma Gleason Grading: Often Disqualifies From Active SurveillancePankaj DubeyNo ratings yet
- Anti-Anginal and Anti-Ischemic DrugsDocument18 pagesAnti-Anginal and Anti-Ischemic DrugsSrisriNo ratings yet