You might also like
- Fistula Politics: Birthing Injuries and the Quest for Continence in NigerFrom EverandFistula Politics: Birthing Injuries and the Quest for Continence in NigerNo ratings yet
- International Surrogacy as Disruptive Industry in Southeast AsiaFrom EverandInternational Surrogacy as Disruptive Industry in Southeast AsiaRating: 5 out of 5 stars5/5 (1)
- Medical Entanglements: Rethinking Feminist Debates about HealthcareFrom EverandMedical Entanglements: Rethinking Feminist Debates about HealthcareNo ratings yet
- Sociocultural Context of Women's Body ImageDocument12 pagesSociocultural Context of Women's Body Imageeftihia_georgiouNo ratings yet
- The Devil's Fruit: Farmworkers, Health, and Environmental JusticeFrom EverandThe Devil's Fruit: Farmworkers, Health, and Environmental JusticeNo ratings yet
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyFrom EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNo ratings yet
- Hps 439a Final Paper 1Document9 pagesHps 439a Final Paper 1api-280707253No ratings yet
- The Menopause: Women's Psychology and Health CareDocument10 pagesThe Menopause: Women's Psychology and Health Carefireni89No ratings yet
- The Politics of Potential: Global Health and Gendered Futures in South AfricaFrom EverandThe Politics of Potential: Global Health and Gendered Futures in South AfricaNo ratings yet
- Homelessness and Menstruation: The Lived Experience of Homeless Women in AdelaideDocument6 pagesHomelessness and Menstruation: The Lived Experience of Homeless Women in AdelaidesofiNo ratings yet
- Abortion Pills, Test Tube Babies, and Sex Toys: Emerging Sexual and Reproductive Technologies in the Middle East and North AfricaFrom EverandAbortion Pills, Test Tube Babies, and Sex Toys: Emerging Sexual and Reproductive Technologies in the Middle East and North AfricaNo ratings yet
- Dying to Count: Post-Abortion Care and Global Reproductive Health Politics in SenegalFrom EverandDying to Count: Post-Abortion Care and Global Reproductive Health Politics in SenegalNo ratings yet
- Calling Family: Digital Technologies and the Making of Transnational Care CollectivesFrom EverandCalling Family: Digital Technologies and the Making of Transnational Care CollectivesNo ratings yet
- Rx Appalachia: Stories of Treatment and Survival in Rural KentuckyFrom EverandRx Appalachia: Stories of Treatment and Survival in Rural KentuckyNo ratings yet
- Pdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionDocument9 pagesPdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionKathyAnnNo ratings yet
- Women's Empowerment and Global Health: A Twenty-First-Century AgendaFrom EverandWomen's Empowerment and Global Health: A Twenty-First-Century AgendaNo ratings yet
- Psychosocial Adjustment Needs of Menopausal Women: Dimkpa, D. IDocument15 pagesPsychosocial Adjustment Needs of Menopausal Women: Dimkpa, D. Ichie_8866No ratings yet
- Feminism and Family Therapy-A Possible Meeting PointDocument16 pagesFeminism and Family Therapy-A Possible Meeting PointDaniela UrreaNo ratings yet
- Body Wars: Making Peace with Women's Bodies (An Activist's Guide)From EverandBody Wars: Making Peace with Women's Bodies (An Activist's Guide)Rating: 3.5 out of 5 stars3.5/5 (7)
- Psychiatric Encounters: Madness and Modernity in Yucatan, MexicoFrom EverandPsychiatric Encounters: Madness and Modernity in Yucatan, MexicoNo ratings yet
- Week 5 Montgomery - Crosscultural Study of MenstruationDocument35 pagesWeek 5 Montgomery - Crosscultural Study of Menstruationnamanleo2002No ratings yet
- Reproductive Disruptions: Gender, Technology, and Biopolitics in the New MillenniumFrom EverandReproductive Disruptions: Gender, Technology, and Biopolitics in the New MillenniumNo ratings yet
- Gender Gaps, Gender Traps Sexual Identity and Vulnerability ToDocument15 pagesGender Gaps, Gender Traps Sexual Identity and Vulnerability ToThành Đạt Lại (Steve)No ratings yet
- PDFDocument23 pagesPDFJudas FK TadeoNo ratings yet
- Ali Et Al, 2011 Gender Roles and Their Influence On Life Prospects For Women in Urban Karachi PakistanDocument10 pagesAli Et Al, 2011 Gender Roles and Their Influence On Life Prospects For Women in Urban Karachi PakistanAyesha BanoNo ratings yet
- Fault Lines of Care: Gender, HIV, and Global Health in BoliviaFrom EverandFault Lines of Care: Gender, HIV, and Global Health in BoliviaNo ratings yet
- Assembling Harriet Martineau's Gender and Health JigsawDocument12 pagesAssembling Harriet Martineau's Gender and Health Jigsawroyhiranmay94No ratings yet
- Healing The Body Through Awareness and Expression The PolyvagalDocument35 pagesHealing The Body Through Awareness and Expression The Polyvagalbordian georgeNo ratings yet
- Life SatisfactionDocument15 pagesLife Satisfactionfernandez.s1299No ratings yet
- Legitimating Life: Adoption in the Age of Globalization and BiotechnologyFrom EverandLegitimating Life: Adoption in the Age of Globalization and BiotechnologyNo ratings yet
- Chapter 2: Overview of LiteratureDocument18 pagesChapter 2: Overview of LiteratureSakshi SharmaNo ratings yet
- 2008 Philippine PovertyDocument14 pages2008 Philippine Povertydelacerna.136504130239No ratings yet
- Chronic Failures: Kidneys, Regimes of Care, and the Mexican StateFrom EverandChronic Failures: Kidneys, Regimes of Care, and the Mexican StateNo ratings yet
- Fielding Miller2020Document13 pagesFielding Miller2020ucan fajrinNo ratings yet
- Life of The MindDocument22 pagesLife of The Mindhowarda09No ratings yet
- Gender Identity in Informal Care: Impact On Health in Spanish CaregiversDocument15 pagesGender Identity in Informal Care: Impact On Health in Spanish CaregiversAUCANLATINMAILNo ratings yet
- Philpov Internationalperspectives PDFDocument21 pagesPhilpov Internationalperspectives PDFelaine faithNo ratings yet
- Those Who Were Born Poor: A Qualitative Study of Philippine PovertyDocument21 pagesThose Who Were Born Poor: A Qualitative Study of Philippine PovertyDea AlviorNo ratings yet
- Sophia RDocument3 pagesSophia Rapi-456983151No ratings yet
- Violence Against Women-2011-Peled-457-79 PDFDocument24 pagesViolence Against Women-2011-Peled-457-79 PDFAnotherAnonymom100% (1)
- Our Bodies, Ourselves: MenopauseFrom EverandOur Bodies, Ourselves: MenopauseRating: 4 out of 5 stars4/5 (10)
- Feminization of PovertyDocument12 pagesFeminization of PovertyPb 29 Speaker 1No ratings yet
- Making Uncertainty: Tuberculosis, Substance Use, and Pathways to Health in South AfricaFrom EverandMaking Uncertainty: Tuberculosis, Substance Use, and Pathways to Health in South AfricaNo ratings yet
- Feminist Agroecology Analyzing Power Relationships in Food SystemsDocument21 pagesFeminist Agroecology Analyzing Power Relationships in Food SystemsClaudia FernándezNo ratings yet
- Starving Is The Most Fun A Girl Can Have'Document16 pagesStarving Is The Most Fun A Girl Can Have'Criis OliveiraNo ratings yet
- Cultural Anxieties: Managing Migrant Suffering in FranceFrom EverandCultural Anxieties: Managing Migrant Suffering in FranceNo ratings yet
- Depressive Symptomatology Among HIV-Positive Women in The Era of HAART: A Stress and Coping ModelDocument12 pagesDepressive Symptomatology Among HIV-Positive Women in The Era of HAART: A Stress and Coping ModelAudia SurachminNo ratings yet
- articlereviewDocument4 pagesarticlereviewGretchen GonzagaNo ratings yet
- Interwoven Threads: Occupational Therapy, Feminism, and Holistic HealthDocument7 pagesInterwoven Threads: Occupational Therapy, Feminism, and Holistic HealthVanesaNo ratings yet
- 1986 - Lock - AMBIQUITIES OF AGING JAPANESE EXPERIENCE AND PERCEPTIONS OF MENOPAUSEDocument24 pages1986 - Lock - AMBIQUITIES OF AGING JAPANESE EXPERIENCE AND PERCEPTIONS OF MENOPAUSEHenrique QuagliatoNo ratings yet
- 2004 Social Inequality and Depressive Disorders in Bahia, Brazil - Interactions of Gender, Ethnicity, and Social ClassDocument15 pages2004 Social Inequality and Depressive Disorders in Bahia, Brazil - Interactions of Gender, Ethnicity, and Social ClassNaomar Almeida-FilhoNo ratings yet
- That Mystery Illness: Michael L. Tan @inquirerdotnetDocument2 pagesThat Mystery Illness: Michael L. Tan @inquirerdotnetMary UyNo ratings yet
- Body Ritual Among The NaciremaDocument6 pagesBody Ritual Among The NaciremaMary UyNo ratings yet
- Pasma 1 and 2. Michael Tan. Pinoy Kasi, Philippine Daily InquirerDocument5 pagesPasma 1 and 2. Michael Tan. Pinoy Kasi, Philippine Daily InquirerMary UyNo ratings yet
- Clean Air Act (CAA) What Is The Clean Air Act?Document11 pagesClean Air Act (CAA) What Is The Clean Air Act?Mary UyNo ratings yet
- MymyDocument1 pageMymyMary UyNo ratings yet
- 3rd Year CurriculumDocument1 page3rd Year CurriculumMary UyNo ratings yet
- FeminismDocument1 pageFeminismMary UyNo ratings yet
- Pathfinder PharmacyInternship Sy1314Document3 pagesPathfinder PharmacyInternship Sy1314Mary UyNo ratings yet
- Secretary's CertificateDocument2 pagesSecretary's CertificateMary Uy60% (10)
- Future PharmacistDocument1 pageFuture PharmacistMary UyNo ratings yet
- P. Falciparum, P. Vivax, P. Ovale, P. Malariae: Blood and Tissue ParasitesDocument1 pageP. Falciparum, P. Vivax, P. Ovale, P. Malariae: Blood and Tissue ParasitesMary UyNo ratings yet
- Future PharmacistDocument1 pageFuture PharmacistMary UyNo ratings yet
- Psychoanalytic TheoryDocument4 pagesPsychoanalytic TheoryMonika JosephNo ratings yet
- Depression in Older AdultsDocument9 pagesDepression in Older Adultsapi-509881562No ratings yet
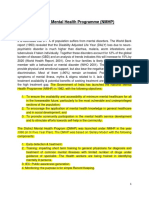
- National Mental Health Programme (NMHP) OverviewDocument19 pagesNational Mental Health Programme (NMHP) OverviewPratibha LoarNo ratings yet
- Attachment 23.3 Personality Diagnostic Questionnaire (PDQ4+) PDFDocument12 pagesAttachment 23.3 Personality Diagnostic Questionnaire (PDQ4+) PDFHerberth MirandaNo ratings yet
- Students List PG PH.D UG Nov 2021Document7 pagesStudents List PG PH.D UG Nov 2021Ashwat ANo ratings yet
- 2018 East Bay Year-Long Psychoanalysis ProgramDocument5 pages2018 East Bay Year-Long Psychoanalysis ProgramVictor GanNo ratings yet
- John Keith Krebs 1 SubstanceAbuse UnjustifiedPrescriptions PDFDocument30 pagesJohn Keith Krebs 1 SubstanceAbuse UnjustifiedPrescriptions PDFWKYC.comNo ratings yet
- Developmental TA & Psychotherapy TA: Similarities & DifferencesDocument24 pagesDevelopmental TA & Psychotherapy TA: Similarities & DifferencesdiaahaNo ratings yet
- Mental Health in USDocument376 pagesMental Health in USmycatholicvoice.comNo ratings yet
- Lex-Mental HealthDocument49 pagesLex-Mental HealthnasimhsNo ratings yet
- Avoidant Personality Disorder Symptoms and TreatmentsDocument4 pagesAvoidant Personality Disorder Symptoms and TreatmentsAngelo ProvidoNo ratings yet
- Glover - The Therapeutic Effect of Inexact InterpretationDocument16 pagesGlover - The Therapeutic Effect of Inexact InterpretationHugo Tannous JorgeNo ratings yet
- David DeBerardinis - Report and Recommendation - April 3 2020Document36 pagesDavid DeBerardinis - Report and Recommendation - April 3 2020shreveporttimesNo ratings yet
- Case Study in Psychoanalysis: Insomnia and InheritanceDocument4 pagesCase Study in Psychoanalysis: Insomnia and InheritanceemofreeNo ratings yet
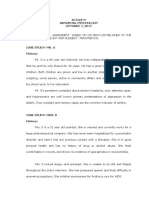
- Activity10 7 17Document11 pagesActivity10 7 17Charlotte GallegoNo ratings yet
- Looking For Information On JournalDocument992 pagesLooking For Information On JournalJames Alejo MuñozNo ratings yet
- Psychodynamic Interpersonal Therapy For Substance Use DisordersDocument11 pagesPsychodynamic Interpersonal Therapy For Substance Use DisordersFrancesca PalazzoloNo ratings yet
- MWF Community Resource Guide - Atlanta - 2014Document32 pagesMWF Community Resource Guide - Atlanta - 2014MuslimWellnessNo ratings yet
- DSM-5 Criteria for PTSDDocument1 pageDSM-5 Criteria for PTSDMarial JavierNo ratings yet
- UntitledDocument455 pagesUntitledEmier Zulhilmi100% (2)
- SElf Directed RT Manic Excitement NCP BM DISORDERDocument2 pagesSElf Directed RT Manic Excitement NCP BM DISORDEREden Marie FranciscoNo ratings yet
- Ditrich 2021Document12 pagesDitrich 2021Felipe CafureNo ratings yet
- Caring for Dementia PatientsDocument4 pagesCaring for Dementia PatientsDerick RanaNo ratings yet
- Scientific Reports Volume 8 Issue 1 2018 (Doi 10.1038/s41598-018-20295-3) Mak, Arthur D. P. Lau, Domily T. Y. Chan, Alicia K. W. So, Su - Cognitive Impairment in Treatment-Naïve Bipolar II and UDocument8 pagesScientific Reports Volume 8 Issue 1 2018 (Doi 10.1038/s41598-018-20295-3) Mak, Arthur D. P. Lau, Domily T. Y. Chan, Alicia K. W. So, Su - Cognitive Impairment in Treatment-Naïve Bipolar II and UArhip CojocNo ratings yet
- Prevalence of Behavioral Disorders Among OrphansDocument7 pagesPrevalence of Behavioral Disorders Among OrphansEricka GutiérrezNo ratings yet
- Add-On Lithium For The Treatment of Unipolar Depression - Too Often ForgottenDocument2 pagesAdd-On Lithium For The Treatment of Unipolar Depression - Too Often Forgottenjuan_bacha_1No ratings yet
- CIDCO Convention Centre, Opp - Vashi Rly Station, Navi MumbaiDocument4 pagesCIDCO Convention Centre, Opp - Vashi Rly Station, Navi MumbaiIslam ForeverNo ratings yet
- Manual - of - Operations - Drug Abuse TreatmentDocument26 pagesManual - of - Operations - Drug Abuse TreatmentmokfreeNo ratings yet
- Nursing Diagnosis Impaired Gas ExchangeDocument7 pagesNursing Diagnosis Impaired Gas ExchangeZycon Rodney Ae'zecquel Gachallan50% (2)
- Data BaseDocument93 pagesData BasebraintreedesignNo ratings yet