You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
- GYNE 4.04 Pelvic Organ DisordersDocument7 pagesGYNE 4.04 Pelvic Organ DisordersGray SnellNo ratings yet
- NBH Truth About HormonesDocument8 pagesNBH Truth About HormonesNaturalBioHealthNo ratings yet
- Test 3 4 5Document8 pagesTest 3 4 5Sayani BanerjeeNo ratings yet
- FIGO 2018 - Cervical CADocument15 pagesFIGO 2018 - Cervical CAJP RecioNo ratings yet
- Ospe Exam O&gDocument43 pagesOspe Exam O&gNabilah Mohammad KhalisNo ratings yet
- Obstetrics and Gynecology Question Papers - Vol IIDocument19 pagesObstetrics and Gynecology Question Papers - Vol IIprinceejNo ratings yet
- Hysterectomy and Bilateral Salpingo-OophorectomyDocument1 pageHysterectomy and Bilateral Salpingo-Oophorectomyapi-3712326100% (3)
- Uterine Fibroids: An Update On Current and Emerging Medical Treatment OptionsDocument22 pagesUterine Fibroids: An Update On Current and Emerging Medical Treatment OptionsAlfian Rahman HadiNo ratings yet
- Medical Treatment of Uterine Leiomyoma: Mohamed Sabry, MD, MSC, RDMS, and Ayman Al-Hendy, MD, PHD, FRCSC, FacogDocument15 pagesMedical Treatment of Uterine Leiomyoma: Mohamed Sabry, MD, MSC, RDMS, and Ayman Al-Hendy, MD, PHD, FRCSC, FacogAlfian Rahman HadiNo ratings yet
- A Short Review of Malabsorption and Anemia: Javier P Gisbert, Professor Fernando Gomollón, MD, PHDDocument9 pagesA Short Review of Malabsorption and Anemia: Javier P Gisbert, Professor Fernando Gomollón, MD, PHDAlfian Rahman HadiNo ratings yet
- Lymph Node GroupsDocument7 pagesLymph Node GroupsAlfian Rahman HadiNo ratings yet
- Hysterectomy - Abdominal - Bilateral - SO PDFDocument2 pagesHysterectomy - Abdominal - Bilateral - SO PDFkatNo ratings yet
- 2009 Fee ScheduleDocument1,123 pages2009 Fee ScheduleNicole HillNo ratings yet
- Holly TranzorDocument2 pagesHolly Tranzorapi-26246128No ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo-Oophorectomy (TAHBSO)Document4 pagesTotal Abdominal Hysterectomy Bilateral Salpingo-Oophorectomy (TAHBSO)mikeraz11011No ratings yet
- Steinberg 2009Document7 pagesSteinberg 2009majedNo ratings yet
- Hysterectomy For Gynecological Indication in Six Medical Facilities in LubumbashiDRC Frequency, Indications, Early Operative ComplicationsDocument11 pagesHysterectomy For Gynecological Indication in Six Medical Facilities in LubumbashiDRC Frequency, Indications, Early Operative ComplicationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
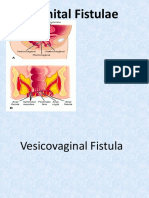
- Fistula GenitaliaDocument35 pagesFistula GenitaliaFifi FruitasariNo ratings yet
- Best Practices For Repair of Iatrogenic Bladder INJURYDocument7 pagesBest Practices For Repair of Iatrogenic Bladder INJURYdlmejiapNo ratings yet
- Vaginal HysterectomyDocument2 pagesVaginal HysterectomymangawatayogpantyNo ratings yet
- Hysterectomy: Frequently Asked Questions FAQ008 Special ProceduresDocument4 pagesHysterectomy: Frequently Asked Questions FAQ008 Special ProceduresGrace Noviyanthi SinambelaNo ratings yet
- Review Article: Uterine Prolapse: From Antiquity To TodayDocument10 pagesReview Article: Uterine Prolapse: From Antiquity To TodayTeguh Adi PartamaNo ratings yet
- Hujiolgy Workstation D05Document6 pagesHujiolgy Workstation D05G.330No ratings yet
- HysterectomyDocument131 pagesHysterectomy8690402592No ratings yet
- Gynaecology Surgery PresentationDocument117 pagesGynaecology Surgery Presentationnorhafizahstoh89No ratings yet
- Gynacology Oncology Glubran2Document5 pagesGynacology Oncology Glubran2atheer gemitalyNo ratings yet
- Symptom Experience in WomenAfter HysterectomyDocument9 pagesSymptom Experience in WomenAfter HysterectomySuci RahmayeniNo ratings yet
- Pelvic Organ ProlapseDocument3 pagesPelvic Organ ProlapseMelissa Aina Mohd YusofNo ratings yet
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaadNo ratings yet
- MM Ob Gyn Catalog WebDocument100 pagesMM Ob Gyn Catalog Webthumper2madNo ratings yet
- MS ObgyDocument18 pagesMS ObgySushantaNo ratings yet
- Endometrial Ablation Experience in SFHDocument36 pagesEndometrial Ablation Experience in SFHElham MNo ratings yet
- Annotated Bibliography Final DraftDocument14 pagesAnnotated Bibliography Final DraftlyrichardNo ratings yet