You might also like
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
- The Journal For Nurse PractitionersDocument5 pagesThe Journal For Nurse Practitionersagstri lestariNo ratings yet
- COVID-19 Disease: Assessment of A Critically Ill Patient: Key PointsDocument8 pagesCOVID-19 Disease: Assessment of A Critically Ill Patient: Key PointsMNurmadani MuhammadNurNo ratings yet
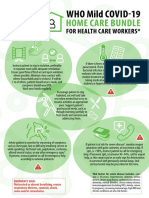
- WHO COVID-19-Home-Care-BundleDocument2 pagesWHO COVID-19-Home-Care-BundleOCSAF - P2LT PUNSALAN MCNo ratings yet
- A Structured Tool For Communication and Care PlannDocument5 pagesA Structured Tool For Communication and Care PlannTari AudinaNo ratings yet
- Pandemic Palliative Care: Beyond Ventilators and Saving LivesDocument5 pagesPandemic Palliative Care: Beyond Ventilators and Saving Livesharvey moncayoNo ratings yet
- Spinal Muscular Atrophy Care in The COVID-19 Pandemic EraDocument4 pagesSpinal Muscular Atrophy Care in The COVID-19 Pandemic EraAriane de Senna PoltozziNo ratings yet
- SMW 2020 20233Document2 pagesSMW 2020 20233Alicia MoraNo ratings yet
- Palliative Care Pandemic Pack A Specialist Palliativ - 2020 - Journal of Pain ADocument3 pagesPalliative Care Pandemic Pack A Specialist Palliativ - 2020 - Journal of Pain AIndiara MartinsNo ratings yet
- Primarna Zdravstvena Zaćštita CovidDocument6 pagesPrimarna Zdravstvena Zaćštita CovidPetar PanNo ratings yet
- C Ovid Patient Treatment GuideDocument29 pagesC Ovid Patient Treatment Guidemmms25No ratings yet
- Hemodialysis Unit Preparedness COVID-19 Pandemic: During and AfterDocument8 pagesHemodialysis Unit Preparedness COVID-19 Pandemic: During and Afteryanuar esthoNo ratings yet
- Uncertainty and COVID-19Document6 pagesUncertainty and COVID-19Arthur FernandesNo ratings yet
- Sedation, Analgesia, and Paralysis in COVID-19 Patients in The Setting of Drug ShortagesDocument18 pagesSedation, Analgesia, and Paralysis in COVID-19 Patients in The Setting of Drug ShortagesPriscila Navarro MedinaNo ratings yet
- 6MINUTEWALKTESTABERTODocument5 pages6MINUTEWALKTESTABERTOpv7j8j6q5rNo ratings yet
- Home Care For Patients With COVID-19 Presenting With Mild Symptoms and Management of Their ContactsDocument5 pagesHome Care For Patients With COVID-19 Presenting With Mild Symptoms and Management of Their ContactsNur MaliaNo ratings yet
- PIIS0140673620310679Document3 pagesPIIS0140673620310679JohnStrowskyNo ratings yet
- COVID - 19 Situation Updat-1Document18 pagesCOVID - 19 Situation Updat-1Elteyb Nor eldaimNo ratings yet
- As Preventive TherapyDocument6 pagesAs Preventive TherapymutimutimutiNo ratings yet
- CCRH - Revised Guidelines For Homeopathy Practitioners For Home Isolated COVID 19 Patient-FDocument4 pagesCCRH - Revised Guidelines For Homeopathy Practitioners For Home Isolated COVID 19 Patient-FTisil KodithottamNo ratings yet
- Papers Intervencion CovidDocument6 pagesPapers Intervencion Coviddayllyn iglesiasNo ratings yet
- Antenatal Care During The COVID-19 Pandemic: Original Research ArticleDocument5 pagesAntenatal Care During The COVID-19 Pandemic: Original Research ArticleAita Utsukushi HyuugaNo ratings yet
- Safari - 12 May 2020 10.04Document1 pageSafari - 12 May 2020 10.04tenun witaNo ratings yet
- Ways of Knowing in NursingDocument4 pagesWays of Knowing in NursingHannah Marice GuintoNo ratings yet
- 0221 Community-Acquired-PneumoniaDocument29 pages0221 Community-Acquired-PneumoniaDiego YanezNo ratings yet
- Dementia and COVID-19 Lockdown More Than A Double Blow For Patients and CaregiversDocument5 pagesDementia and COVID-19 Lockdown More Than A Double Blow For Patients and CaregiversIraNo ratings yet
- WHO Covid19 HomeCare 2020.3 EngDocument4 pagesWHO Covid19 HomeCare 2020.3 EngReggie CastroNo ratings yet
- Care For Critically Ill Patients With COVID-19: Clinical UpdateDocument2 pagesCare For Critically Ill Patients With COVID-19: Clinical UpdateNicole BatistaNo ratings yet
- The Central Role of Clinical Nutrition in COVID-19 Patients During and After Hospitalization in Intensive Care UnitDocument5 pagesThe Central Role of Clinical Nutrition in COVID-19 Patients During and After Hospitalization in Intensive Care UnitReaz MorshedNo ratings yet
- Clinical PracticeDocument10 pagesClinical PracticeCarlos AlvarezNo ratings yet
- Chiappini 2021Document7 pagesChiappini 2021Arumm88No ratings yet
- Whats New in GINA 2021 - Final - V2Document52 pagesWhats New in GINA 2021 - Final - V2Wialda Dwi rodyahNo ratings yet
- Journal of The Neurological Sciences: Clinical Short CommunicationDocument3 pagesJournal of The Neurological Sciences: Clinical Short CommunicationMartha OktaviaNo ratings yet
- Humanism in The Age of COVID-19Document5 pagesHumanism in The Age of COVID-19Jhoelis SalazarNo ratings yet
- Current Scenario For Management On Covid-19 - A Global Review Indra S, Vijayasankari A, Kalpana SDocument5 pagesCurrent Scenario For Management On Covid-19 - A Global Review Indra S, Vijayasankari A, Kalpana Snithish krishnaNo ratings yet
- Saint - Lucia COVID-19 Community ManagenentDocument18 pagesSaint - Lucia COVID-19 Community ManagenentOqba AlzwainyNo ratings yet
- Critical Care Lecture NotesDocument10 pagesCritical Care Lecture Notesapi-280066855No ratings yet
- Coronavirus On The Inpatient Unit: A New Challenge For Psychiatry - MDedge PsychiatryDocument3 pagesCoronavirus On The Inpatient Unit: A New Challenge For Psychiatry - MDedge PsychiatryAKNTAI002No ratings yet
- 5 Family Medicine in Times of COVID 19 A Generalists VoiceDocument4 pages5 Family Medicine in Times of COVID 19 A Generalists VoiceVANESSA GLORIA POLIINo ratings yet
- Jama Murthy 2020 It 200008Document2 pagesJama Murthy 2020 It 200008jorgeNo ratings yet
- Guias JamaDocument2 pagesGuias JamaEliana TorresNo ratings yet
- 415 2020 Article 9898Document2 pages415 2020 Article 9898gevowo3277No ratings yet
- The Family Caregiving Crisis Meets An Actual Pandemic: ResearchDocument4 pagesThe Family Caregiving Crisis Meets An Actual Pandemic: ResearchMila KhanifaNo ratings yet
- Locke 2016 Diários X PICSDocument9 pagesLocke 2016 Diários X PICSGabriela LealNo ratings yet
- Referensi 47Document7 pagesReferensi 47SaebaNo ratings yet
- First Case Report of A Successfully Managed Severe COVID-19 Infectionin MalawiDocument4 pagesFirst Case Report of A Successfully Managed Severe COVID-19 Infectionin MalawiYoga PrabawaNo ratings yet
- Mitigating Risk of COVID-19 in Dialysis Facilities: Alan S. Kliger and Jeffrey SilberzweigDocument3 pagesMitigating Risk of COVID-19 in Dialysis Facilities: Alan S. Kliger and Jeffrey SilberzweigRChofiyana OchiNo ratings yet
- The Lived Experience of Filipino Nurses' Work in COVID-19 Quarantine Facilities: A Descriptive Phenomenological StudyDocument11 pagesThe Lived Experience of Filipino Nurses' Work in COVID-19 Quarantine Facilities: A Descriptive Phenomenological StudyAldrin Zolina100% (1)
- Coronavirus Disease 2019 (COVID-19) in Brasil: Information To Physical TherapistsDocument4 pagesCoronavirus Disease 2019 (COVID-19) in Brasil: Information To Physical TherapistsandctzgNo ratings yet
- NEWS2 v2 - 0Document1 pageNEWS2 v2 - 0seni arcanaashkaNo ratings yet
- NEWS2 v2 - 0 PDFDocument1 pageNEWS2 v2 - 0 PDFblount juniorNo ratings yet
- Severe Covid-19: Clinical PracticeDocument10 pagesSevere Covid-19: Clinical Practicemarcelocarvalhoteacher2373No ratings yet
- Radiation 1Document3 pagesRadiation 1elite internationalNo ratings yet
- Journal Pre-Proof: Journal of Geriatric OncologyDocument6 pagesJournal Pre-Proof: Journal of Geriatric OncologySteven FloresNo ratings yet
- RHD CovidDocument2 pagesRHD CovidHana Nuraisa BasyaNo ratings yet
- Evolution of Acute Respiratory Distress Syndrome IDocument14 pagesEvolution of Acute Respiratory Distress Syndrome InalgatronNo ratings yet
- Critical Care of Patient With Covid 19Document32 pagesCritical Care of Patient With Covid 19Anonymous Kv0sHqFNo ratings yet
- Soluciones de VIDocument2 pagesSoluciones de VILailaNo ratings yet
- DCCN 40 156Document8 pagesDCCN 40 156liyana SyatirahNo ratings yet
- John Taylor Case Study ENP and EPPDocument11 pagesJohn Taylor Case Study ENP and EPPAhata Sham NewazNo ratings yet
- Fitness Calculator Python ProjectDocument12 pagesFitness Calculator Python ProjectNishitha NeelamNo ratings yet
- USHK - A - Clean - Environment - Healthy - Me - EngDocument24 pagesUSHK - A - Clean - Environment - Healthy - Me - EngBeaa BeaaNo ratings yet
- Kinesiology Tape Guide - Physix Gear Sport PDFDocument85 pagesKinesiology Tape Guide - Physix Gear Sport PDFTomas Delfiner100% (1)
- Speech by Deputy Minister Mhaule at Media Briefing 15 January 2021.finalDocument5 pagesSpeech by Deputy Minister Mhaule at Media Briefing 15 January 2021.finaleNCA.comNo ratings yet
- Mouse DissectionDocument6 pagesMouse DissectionMauricio F. VillamarNo ratings yet
- EO 70 S. 2021 - Movement of Pigs and Pork Products ASF-DSDocument8 pagesEO 70 S. 2021 - Movement of Pigs and Pork Products ASF-DSJamela SerutNo ratings yet
- Pratiwi S Gunawan, BDS., DDS., MDSC, PHDDocument53 pagesPratiwi S Gunawan, BDS., DDS., MDSC, PHDBima Ewando KabanNo ratings yet
- Notice: Grants and Cooperative Agreements Availability, Etc.: Women Living in Puerto Rico and U.S. Virgin Islands HIV Prevention ProgramDocument8 pagesNotice: Grants and Cooperative Agreements Availability, Etc.: Women Living in Puerto Rico and U.S. Virgin Islands HIV Prevention ProgramJustia.comNo ratings yet
- HIV in South AfricaDocument17 pagesHIV in South AfricaMadelineNo ratings yet
- Barneys Farm SeedsDocument46 pagesBarneys Farm SeedsPedro MarquesNo ratings yet
- Final Draft of Interview TranscriptDocument7 pagesFinal Draft of Interview Transcriptapi-549369201No ratings yet
- Phlegmon: by - Dharmendra Singh Group No. - 317Document15 pagesPhlegmon: by - Dharmendra Singh Group No. - 317Mouna Jomaa DhifaouiNo ratings yet
- Pet Food 2Document73 pagesPet Food 2AB100% (1)
- Nosebleed and PoisoningDocument28 pagesNosebleed and PoisoningRenz100% (2)
- Osce ChecklistDocument11 pagesOsce Checklistgemgem06No ratings yet
- Chapter 8 Blood Group Terminology and The Other Blood GroupsDocument62 pagesChapter 8 Blood Group Terminology and The Other Blood GroupsschemologyNo ratings yet
- Pat An AnewDocument126 pagesPat An AnewgshchurovskiyNo ratings yet
- Insidens Dan Karakteristik Kelainan Kongenital Traktus Gastrointestinal Pada Neonatus Di Rumah Sakit Umum Pusat Sanglah Denpasar Tahun 2015Document5 pagesInsidens Dan Karakteristik Kelainan Kongenital Traktus Gastrointestinal Pada Neonatus Di Rumah Sakit Umum Pusat Sanglah Denpasar Tahun 2015Noval HidayatNo ratings yet
- Environmental Hazards Assignment Winter Quarter 2015-16Document32 pagesEnvironmental Hazards Assignment Winter Quarter 2015-16Muhammad AbbasNo ratings yet
- Other Products of ChesaDocument4 pagesOther Products of ChesamikeeNo ratings yet
- Bach Flowers CombinationsDocument20 pagesBach Flowers Combinationsraghavan remidicharla100% (3)
- Ada CambraDocument7 pagesAda CambraCristiano Pereira AlvesNo ratings yet
- LEC-3 Telemedicine & Medical Informatics: By: Abdul Hanan TaqiDocument9 pagesLEC-3 Telemedicine & Medical Informatics: By: Abdul Hanan TaqiAbdul RaufNo ratings yet
- 02 - Recalibrating Gavi 5.0 in Light of COVID-19 and Successful Replenis..Document19 pages02 - Recalibrating Gavi 5.0 in Light of COVID-19 and Successful Replenis..aman_sasanNo ratings yet
- Myocardial InfarctionDocument34 pagesMyocardial InfarctionMeera ANN AJINo ratings yet
- Script For OrientationDocument2 pagesScript For OrientationAngela CudiaNo ratings yet
- Neonatal SepsisDocument6 pagesNeonatal SepsisSunaina AdhikariNo ratings yet
- Bright Adjei B.A. (Hons.)Document136 pagesBright Adjei B.A. (Hons.)gideon A. owusuNo ratings yet
- 1187 FullDocument7 pages1187 FullPrincessDianna SulitNo ratings yet
- Medical Revision PaperDocument106 pagesMedical Revision PaperDavin SugumarNo ratings yet