You might also like
- Nur1 230 Fundamentals of Canadian NursingDocument1,666 pagesNur1 230 Fundamentals of Canadian NursingSamantha Lau100% (4)
- Basic Surgical Skills 2014Document108 pagesBasic Surgical Skills 2014Mi Zulfahmi Sha'ari100% (1)
- Osce SuturingDocument3 pagesOsce Suturingdaniel ragonjanNo ratings yet
- Suture Practice Kit GuideDocument18 pagesSuture Practice Kit GuideKarla Aguilar GuerreroNo ratings yet
- BSS GP 2020Document60 pagesBSS GP 2020adi10 adi10No ratings yet
- Basic Surgical Skills Indonesia 2016Document17 pagesBasic Surgical Skills Indonesia 2016'putu' AcaaRyaaNo ratings yet
- Bss1 - Indonesia - Share2018Document43 pagesBss1 - Indonesia - Share2018Michael RaktionNo ratings yet
- BSS For GP IndonesiaDocument25 pagesBSS For GP IndonesiaSayed Saiful WajirNo ratings yet
- Basic surgical skills for Indonesia 2018Document25 pagesBasic surgical skills for Indonesia 2018Andi MulyawanNo ratings yet
- 1556014154-BSS GP Indonesia 2019Document24 pages1556014154-BSS GP Indonesia 2019Zuldi ErdiansyahNo ratings yet
- BSS 2018Document24 pagesBSS 2018gumoha01No ratings yet
- Abscess Incision and Drainage - Examiner RoleplayDocument5 pagesAbscess Incision and Drainage - Examiner Roleplaysanju ghimireNo ratings yet
- Proper Bandaging TechniquesDocument13 pagesProper Bandaging TechniquesAnkita Bramhe100% (1)
- De La Salle Medical College Suturing GuideDocument6 pagesDe La Salle Medical College Suturing GuideNehemiah FranciscoNo ratings yet
- Basic Surgical Skills Indonesia 2019Document25 pagesBasic Surgical Skills Indonesia 2019Sri MahadhanaNo ratings yet
- Bandaging Demo 2Document21 pagesBandaging Demo 2Janie GraceNo ratings yet
- Bandaging: Presented By: Sumati Singh M. Sc. Nursing 1 YearDocument35 pagesBandaging: Presented By: Sumati Singh M. Sc. Nursing 1 YearNedhi Singh100% (2)
- Oral Surgery, Sheet9, DR - SukaynaDocument11 pagesOral Surgery, Sheet9, DR - SukaynamzusaqNo ratings yet
- 4 Suturing MaterialDocument41 pages4 Suturing MaterialAdimera TsehayeNo ratings yet
- Surgical Skin Prep and DrapingDocument30 pagesSurgical Skin Prep and DrapingshyluckmayddpNo ratings yet
- BandagingDocument42 pagesBandagingMuhammad Shahzad ChandiaNo ratings yet
- Suturing ClassDocument129 pagesSuturing ClassRajani GedelaNo ratings yet
- Surgical Hand Antisepsis Gowning and Gloving Suturing: Flora AgustinaDocument38 pagesSurgical Hand Antisepsis Gowning and Gloving Suturing: Flora AgustinaFlora AgustinaNo ratings yet
- NCM 107-A # 2Document171 pagesNCM 107-A # 2Contessa GabrielNo ratings yet
- Mohamed Sadiq 2020 Lec 3Document30 pagesMohamed Sadiq 2020 Lec 3ParstarmNo ratings yet
- Basic and Special Suturing Techniques in SurgeryDocument32 pagesBasic and Special Suturing Techniques in SurgeryRobins DhakalNo ratings yet
- Basic Surgical InstrumenDocument36 pagesBasic Surgical InstrumenYoga PribadiNo ratings yet
- What Is Suturing?: - The Primary Objective Is To Position andDocument16 pagesWhat Is Suturing?: - The Primary Objective Is To Position andmehak malhotraNo ratings yet
- Surgical Scrub ProcessDocument23 pagesSurgical Scrub ProcessSHALVI SHARMANo ratings yet
- Lesson 5 Controlling Bleeding 2 - CLSDocument18 pagesLesson 5 Controlling Bleeding 2 - CLSsrtmedicNo ratings yet
- SuturingDocument32 pagesSuturingsobshortNo ratings yet
- Everything You Need to Know About SuturingDocument19 pagesEverything You Need to Know About SuturingSangeeta BSRNo ratings yet
- Asepsi S: SurgicalDocument47 pagesAsepsi S: Surgicalspongebob27No ratings yet
- Basics of Instrument and Tissue HandlingDocument55 pagesBasics of Instrument and Tissue Handlingrutikanaga williamNo ratings yet
- Introduction To First AidDocument61 pagesIntroduction To First AidLim Jun BinNo ratings yet
- Health Assistant ClassDocument47 pagesHealth Assistant ClassAbhishek TandonNo ratings yet
- ASEPSIS: Preventing Infection Through Proper TechniquesDocument36 pagesASEPSIS: Preventing Infection Through Proper TechniquesChevelle Valenciano-GaanNo ratings yet
- Wound dressing and suture care guideDocument20 pagesWound dressing and suture care guideRitaNo ratings yet
- ENG InstrumentsDocument41 pagesENG InstrumentsRoxanaAnaHociungNo ratings yet
- Suturing Materials and TechniquesDocument29 pagesSuturing Materials and Techniquesharshini100% (1)
- Suturing: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing IndiaDocument20 pagesSuturing: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing IndiaNamulondo Mwajib BogereNo ratings yet
- First Aid Dressing BandagesDocument23 pagesFirst Aid Dressing BandagesLawrence cruzanaNo ratings yet
- 1st Aid BandagingDocument35 pages1st Aid BandagingSophia WongNo ratings yet
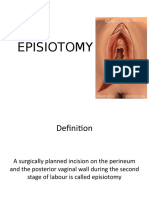
- EPISIOTOMY FinalDocument30 pagesEPISIOTOMY FinalBindu PhilipNo ratings yet
- Basic surgical skills for rural healthcareDocument7 pagesBasic surgical skills for rural healthcareAhmed Reda DoniaNo ratings yet
- General Surgical Instrumentation-1Document26 pagesGeneral Surgical Instrumentation-1ermias UmerNo ratings yet
- Basic Suturing and Wound Management SeminarDocument77 pagesBasic Suturing and Wound Management Seminarpranoto jaconNo ratings yet
- First Aid and BandagingDocument48 pagesFirst Aid and BandagingNor anisa BaguindaNo ratings yet
- How To Assist An OperationDocument41 pagesHow To Assist An OperationDiana IdrisNo ratings yet
- Splinting Techniques: by Madhumitha M, Aruna G, Abi P, Sakthivelayudham G, Sujidha R, Srivignesh MDocument99 pagesSplinting Techniques: by Madhumitha M, Aruna G, Abi P, Sakthivelayudham G, Sujidha R, Srivignesh MSakthivelayudhamganesanNo ratings yet
- Station Exam - Pharm and MedsurgDocument9 pagesStation Exam - Pharm and MedsurgbriannareardonNo ratings yet
- Simple Interrupted Suture (Silicon Skin Pad)Document11 pagesSimple Interrupted Suture (Silicon Skin Pad)Yusuf LawalNo ratings yet
- Surgery CourseDocument28 pagesSurgery CourseAskjsjNo ratings yet
- Affection of Horn: Diseases of Integumentary SystemDocument31 pagesAffection of Horn: Diseases of Integumentary SystemInam khanNo ratings yet
- Asepsis and antisepsis techniques in the operating roomDocument57 pagesAsepsis and antisepsis techniques in the operating roomswestyNo ratings yet
- PT 111 - N Chapter 6: BandagingDocument61 pagesPT 111 - N Chapter 6: BandagingJan Crizza Dale R. FrancoNo ratings yet
- Manual of Ambulatory General Surgery: A Step-by-Step Guide to Minor and Intermediate SurgeryFrom EverandManual of Ambulatory General Surgery: A Step-by-Step Guide to Minor and Intermediate SurgeryNo ratings yet
- Beginning Quilting the Super Simple Way: All the Basics to Get You Started, 15 Projects with Step-by-Step InstructionsFrom EverandBeginning Quilting the Super Simple Way: All the Basics to Get You Started, 15 Projects with Step-by-Step InstructionsNo ratings yet
- Sew Cuddly: 12 Plush Minky Projects for Fun & Fashion—Tips & Techniques to Conquer CuddleFrom EverandSew Cuddly: 12 Plush Minky Projects for Fun & Fashion—Tips & Techniques to Conquer CuddleNo ratings yet
- Introduction To Laparoscopic Surgery: Basic Surgical Skills CourseDocument16 pagesIntroduction To Laparoscopic Surgery: Basic Surgical Skills CourseInomy ClaudiaNo ratings yet
- Effects of Chemotherapy in Breast Cancer PatientsDocument9 pagesEffects of Chemotherapy in Breast Cancer PatientsInomy ClaudiaNo ratings yet
- Modul ELPT Level 2 (20H) - PusbamulyaDocument117 pagesModul ELPT Level 2 (20H) - PusbamulyaRhesa Milzam FavianNo ratings yet
- Sister Mary JosephDocument6 pagesSister Mary JosephInomy ClaudiaNo ratings yet
- IntroductionDocument28 pagesIntroductionInomy ClaudiaNo ratings yet
- Surgical Management of Hemorrhoids: ReviewDocument9 pagesSurgical Management of Hemorrhoids: ReviewInomy ClaudiaNo ratings yet
- 1 Basic Principles in Head & Neck Tumor SurgeryDocument36 pages1 Basic Principles in Head & Neck Tumor SurgeryInomy ClaudiaNo ratings yet
- Diathermy 2019Document18 pagesDiathermy 2019Sri MahadhanaNo ratings yet
- Diathermy 2019Document18 pagesDiathermy 2019Sri MahadhanaNo ratings yet
- Guidelines For The Surgical Treatment of Esophageal Achalasia PDFDocument24 pagesGuidelines For The Surgical Treatment of Esophageal Achalasia PDFInomy ClaudiaNo ratings yet
- Adverse Reactions Following T-Tube Removal: World Journal of SDR RyDocument5 pagesAdverse Reactions Following T-Tube Removal: World Journal of SDR RyInomy ClaudiaNo ratings yet
- Ijcmr 894 3 PDFDocument3 pagesIjcmr 894 3 PDFInomy ClaudiaNo ratings yet
- A Comparative Study of Open (Milligan-Morgan) Versus Closed (Ferguson) HemorrhoidectomyDocument4 pagesA Comparative Study of Open (Milligan-Morgan) Versus Closed (Ferguson) HemorrhoidectomyInomy ClaudiaNo ratings yet
- Incarcerated Groin Hernias in AdultsDocument6 pagesIncarcerated Groin Hernias in AdultsMusthafa Afif WardhanaNo ratings yet
- Watchful Waiting As A Treatment Strategy in Patients With Asymptomatic Inguinal HerniaDocument7 pagesWatchful Waiting As A Treatment Strategy in Patients With Asymptomatic Inguinal HerniaInomy ClaudiaNo ratings yet
- Wainwright2007 PDFDocument13 pagesWainwright2007 PDFInomy ClaudiaNo ratings yet
- Inguinal Hernia Repair: Incidence of Elective and Emergency Surgery, Readmission and MortalityDocument5 pagesInguinal Hernia Repair: Incidence of Elective and Emergency Surgery, Readmission and MortalityInomy ClaudiaNo ratings yet
- HHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesDocument12 pagesHHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesInomy ClaudiaNo ratings yet
- HHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesDocument12 pagesHHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesInomy ClaudiaNo ratings yet
- Oesophageal Motility Disorders SeminarDocument6 pagesOesophageal Motility Disorders SeminarInomy ClaudiaNo ratings yet
- A One Hundred Year Journey: The History of Surgery For Esophageal AchalasiaDocument8 pagesA One Hundred Year Journey: The History of Surgery For Esophageal AchalasiaInomy ClaudiaNo ratings yet
- Updates Surgical Management of Esophageal AchalasiaDocument7 pagesUpdates Surgical Management of Esophageal AchalasiaInomy ClaudiaNo ratings yet
- Pathophysiology of Achalasia: Wai-Kit Lo and Hiroshi MashimoDocument6 pagesPathophysiology of Achalasia: Wai-Kit Lo and Hiroshi MashimoInomy ClaudiaNo ratings yet
- Acalazia CardieiDocument29 pagesAcalazia CardieiIrko SolnyshkoNo ratings yet
- Nutrition in Clinical Practice: Dumping Syndrome: Pathophysiology and TreatmentDocument10 pagesNutrition in Clinical Practice: Dumping Syndrome: Pathophysiology and TreatmentInomy ClaudiaNo ratings yet
- A One Hundred Year Journey: The History of Surgery For Esophageal AchalasiaDocument8 pagesA One Hundred Year Journey: The History of Surgery For Esophageal AchalasiaInomy ClaudiaNo ratings yet
- Flyer SugiesDocument2 pagesFlyer SugiesInomy ClaudiaNo ratings yet
- Wide excision and thoracoabdominal flap closure for recurrent malignant phyllodes tumorDocument1 pageWide excision and thoracoabdominal flap closure for recurrent malignant phyllodes tumorInomy ClaudiaNo ratings yet
- MSDS H2O2 SolvayDocument14 pagesMSDS H2O2 SolvayVedastra AstaNo ratings yet
- SWINE Magazine Feb/Apr 2021Document30 pagesSWINE Magazine Feb/Apr 2021jem ruizNo ratings yet
- UMK Walk-In Interviews Academic & Support Staff PositionsDocument5 pagesUMK Walk-In Interviews Academic & Support Staff PositionsMuis MuliaNo ratings yet
- SBi Guidelines 233 - Protection Against Radon in New BuildingsDocument49 pagesSBi Guidelines 233 - Protection Against Radon in New BuildingsDaniela HanekováNo ratings yet
- Kombucha Fermentation and Its Antimicrobial Activity: KeywordsDocument6 pagesKombucha Fermentation and Its Antimicrobial Activity: KeywordsalirezamdfNo ratings yet
- Avon Fabulous Curls Hair SerumDocument4 pagesAvon Fabulous Curls Hair Serumdenemegaranti78No ratings yet
- HerpesDocument2 pagesHerpesMaria Chacón CarbajalNo ratings yet
- High-Dose Corticosteroids Improve The Prognosis of Bell 'S Palsy Compared With Low-Dose Corticosteroids: A Propensity Score AnalysisDocument6 pagesHigh-Dose Corticosteroids Improve The Prognosis of Bell 'S Palsy Compared With Low-Dose Corticosteroids: A Propensity Score AnalysisRiyanti DeviNo ratings yet
- 1CDDocument99 pages1CDEduardo MuñizNo ratings yet
- Summative 2 Form 2 November K2Document4 pagesSummative 2 Form 2 November K2Sha MinNo ratings yet
- Brittle Bone Disease Causes Fragile BonesDocument30 pagesBrittle Bone Disease Causes Fragile BonesKhim GoyenaNo ratings yet
- Luyen Thi Bai Tap Doc HieuDocument3 pagesLuyen Thi Bai Tap Doc HieuChi MinhNo ratings yet
- SMART Goal SettingDocument5 pagesSMART Goal SettingblakeloganNo ratings yet
- Mem671 Case Study March 2023Document11 pagesMem671 Case Study March 2023AIMAN ASYRAAF BIN ROSLANNo ratings yet
- Syllabus ContentDocument11 pagesSyllabus Contentflower boomNo ratings yet
- Levels of Evidence Flow Chart Rev May 2019Document3 pagesLevels of Evidence Flow Chart Rev May 2019Karl RobleNo ratings yet
- Rapid Real-Time PCR for Diagnosing Tinea InfectionsDocument7 pagesRapid Real-Time PCR for Diagnosing Tinea InfectionsSiti Bellia Arafah XndNo ratings yet
- Paracetamol Use Dec 2008Document30 pagesParacetamol Use Dec 2008Nararto PrijogoNo ratings yet
- SupplementsDocument30 pagesSupplementsAwseome Vaibhav SahrawatNo ratings yet
- Aseptic Dispensing: Bilal Hassan M.Phil PharmaceuticsDocument25 pagesAseptic Dispensing: Bilal Hassan M.Phil PharmaceuticsShafaqat Ghani Shafaqat GhaniNo ratings yet
- PIP LGU MaragondonDocument10 pagesPIP LGU MaragondonAna Riza AndayaNo ratings yet
- COVID-19 Vaccination Hesitancy, Misinformation and Conspiracy Theories On Social Media: A Content Analysis of Twitter DataDocument30 pagesCOVID-19 Vaccination Hesitancy, Misinformation and Conspiracy Theories On Social Media: A Content Analysis of Twitter DataPutri Raudatul JannahNo ratings yet
- Cigna'S Preventive Health Coverage: A Guide ToDocument12 pagesCigna'S Preventive Health Coverage: A Guide TomcrphNo ratings yet
- Safety Data Sheet Corrosive ChemicalDocument2 pagesSafety Data Sheet Corrosive Chemicalzubair1951No ratings yet
- Health Assessment Chapter 1Document4 pagesHealth Assessment Chapter 1Louie Jaie TiredNo ratings yet
- Presented By: MR Jason M BaswelDocument21 pagesPresented By: MR Jason M BaswelJonas valerioNo ratings yet
- Guide: Hybrid Seed Production in TomatoDocument8 pagesGuide: Hybrid Seed Production in TomatoDaniel Rodriguez MartinezNo ratings yet
- Hfi 360Document5 pagesHfi 360Emanuel John BangoNo ratings yet
- Kanada - The Food and Beverage Market Entry HandbookDocument389 pagesKanada - The Food and Beverage Market Entry HandbookWade EtienneNo ratings yet