You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
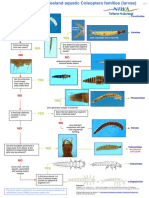
- Quick Guide To Coleoptera Families - LarvaeDocument1 pageQuick Guide To Coleoptera Families - LarvaeLuisCarlosVillarrealDíazNo ratings yet
- 48798-Article Text-147774-159841-10-20190325Document7 pages48798-Article Text-147774-159841-10-20190325LuisCarlosVillarrealDíazNo ratings yet
- Correspondence and Replies: Anne Y. Liu, MDDocument1 pageCorrespondence and Replies: Anne Y. Liu, MDLuisCarlosVillarrealDíazNo ratings yet
- Rodrigues 2001Document14 pagesRodrigues 2001LuisCarlosVillarrealDíazNo ratings yet
- Phycological Reviews 6 Ecology of Soil Algae: A ReviewDocument16 pagesPhycological Reviews 6 Ecology of Soil Algae: A ReviewLuisCarlosVillarrealDíazNo ratings yet
- Mcdowall & Taylor. - Enviromental Indicators of Habitat Quality in A Migratory Freshwater FDocument18 pagesMcdowall & Taylor. - Enviromental Indicators of Habitat Quality in A Migratory Freshwater FLuisCarlosVillarrealDíazNo ratings yet
- Managing Rain-Filled Wetlands For Carbon Sequestration - 2017Document8 pagesManaging Rain-Filled Wetlands For Carbon Sequestration - 2017LuisCarlosVillarrealDíazNo ratings yet
- Diversity of Desmid AlgaeDocument13 pagesDiversity of Desmid AlgaeLuisCarlosVillarrealDíazNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 4 CovidDocument47 pages4 CovidAbhishek toppoNo ratings yet
- Impact of Covid 19 On WorkforceDocument14 pagesImpact of Covid 19 On Workforcejatin girotra100% (1)
- DCSB Response To DOEDocument3 pagesDCSB Response To DOEActionNewsJaxNo ratings yet
- Training On Covid-19 For The Local Task Force: Department of Health, PhilippinesDocument24 pagesTraining On Covid-19 For The Local Task Force: Department of Health, PhilippinesSeriel TismoNo ratings yet
- Asia Society Philippines - Back-to-School - 0Document14 pagesAsia Society Philippines - Back-to-School - 0Christal Daza IINo ratings yet
- Richland County School District 1 COVID ProtocolsDocument1 pageRichland County School District 1 COVID ProtocolsWLTXNo ratings yet
- First DsbdaDocument34 pagesFirst Dsbdauniqueengineer099No ratings yet
- Aviation Industry Leaders Report 2022Document62 pagesAviation Industry Leaders Report 2022Raja Churchill DassNo ratings yet
- Covid Resources HYDDocument24 pagesCovid Resources HYDSurendar SirviNo ratings yet
- Impact of Covid 19 Pandemic Factors Affecting Micro Enterprises in Deciding Whether To Shift Strategies orDocument100 pagesImpact of Covid 19 Pandemic Factors Affecting Micro Enterprises in Deciding Whether To Shift Strategies orKristine Esplana Toralde86% (7)
- COM OBDC Small Biz Stabilization Grant AppDocument7 pagesCOM OBDC Small Biz Stabilization Grant Appdominique marshallNo ratings yet
- Guide Questions:: Diagram 1. COVID-19 Impact Chain, City of Las Piñas, Metro Manila InstructionsDocument39 pagesGuide Questions:: Diagram 1. COVID-19 Impact Chain, City of Las Piñas, Metro Manila Instructionsnilo castroNo ratings yet
- Socioeconomic Impacts of COVID-19: September 2020Document30 pagesSocioeconomic Impacts of COVID-19: September 2020P MarieNo ratings yet
- Will Trump Run Again and Win?: More From AuthorDocument6 pagesWill Trump Run Again and Win?: More From AuthorSyed Sulaiman ShahNo ratings yet
- The Impact of Covid-19 To WomenDocument3 pagesThe Impact of Covid-19 To WomenYsabelle ToradoNo ratings yet
- Statistics Cala... Time SeriesDocument8 pagesStatistics Cala... Time SeriesModina Ruzvidzo100% (1)
- TMAC Special Meeting MICDocument156 pagesTMAC Special Meeting MICOwm Close CorporationNo ratings yet
- CPED Policy Brief Series 2021 No.2Document7 pagesCPED Policy Brief Series 2021 No.2Job EronmhonseleNo ratings yet
- RM Cia 1Document5 pagesRM Cia 1Deepali DeeptiNo ratings yet
- The Impact of COVID-19 in Education - More Than A Year of DisruptionDocument41 pagesThe Impact of COVID-19 in Education - More Than A Year of DisruptionCityPress100% (1)
- Related Studies AyeeeDocument6 pagesRelated Studies AyeeeNoelle CaballeraNo ratings yet
- Colorado COVID-19 Public Health Order April 15, 2021Document7 pagesColorado COVID-19 Public Health Order April 15, 2021Michael_Roberts2019No ratings yet
- The Impact of COVID 19 On The Growing North South DivideDocument9 pagesThe Impact of COVID 19 On The Growing North South Divideსო ფიაNo ratings yet
- Contingency Plan Benito Soliven Central School: My Covid-19 Contingency PlanDocument3 pagesContingency Plan Benito Soliven Central School: My Covid-19 Contingency PlanHeherson S. MarianoNo ratings yet
- Effects of Decreasing Tourist Rate of Travel Destinations To The Residents of Burauen Due To COVID-19 Restrictions (Case Study by Ian Bong Jonale)Document14 pagesEffects of Decreasing Tourist Rate of Travel Destinations To The Residents of Burauen Due To COVID-19 Restrictions (Case Study by Ian Bong Jonale)Rosheine Ann DazoNo ratings yet
- Foreign LiteratureDocument5 pagesForeign Literaturekris jericho buenabilesNo ratings yet
- Four Aviation Security Service Employees V Minister of COVID-19 ResponseDocument2 pagesFour Aviation Security Service Employees V Minister of COVID-19 ResponsepantsNo ratings yet
- OLHS COVID Phase-IV BackToSchool FlyerDocument1 pageOLHS COVID Phase-IV BackToSchool FlyerRachael ThomasNo ratings yet
- Ohio Department of Health's COVID Guidance For K-12 SchoolsDocument13 pagesOhio Department of Health's COVID Guidance For K-12 SchoolsWBNS-TVNo ratings yet
- Gpeople: FactsDocument41 pagesGpeople: FactsChutzpah eduNo ratings yet