You might also like
- Health Care Quality ConceptsDocument11 pagesHealth Care Quality Conceptsmike700usNo ratings yet
- Effective Knowledge Management ModelDocument6 pagesEffective Knowledge Management ModelAika P. BartolomeNo ratings yet
- Change Management Plan - JudahDocument3 pagesChange Management Plan - JudahAmenet JudahNo ratings yet
- HMSWeb - Handover Management SystemDocument21 pagesHMSWeb - Handover Management SystemGG GRNo ratings yet
- Toshiba X-Ray Tube Product InfoDocument10 pagesToshiba X-Ray Tube Product InfoJairo ManzanedaNo ratings yet
- DRW Questions 2Document16 pagesDRW Questions 2Natasha Elena TarunadjajaNo ratings yet
- Strengthening RC Structures with Steel Plate Bonding MethodsDocument29 pagesStrengthening RC Structures with Steel Plate Bonding MethodsSiti Rohani Isdris100% (1)
- BNS Honours Nursing Quality ImprovementDocument14 pagesBNS Honours Nursing Quality ImprovementyeapgyNo ratings yet
- Om 11 Quality ImprovementDocument26 pagesOm 11 Quality ImprovementMochamadAliHaidarNo ratings yet
- LeanDocument38 pagesLeanFadi SalahNo ratings yet
- Quality Assurence in Obstetrical and Gynaecological UnitDocument10 pagesQuality Assurence in Obstetrical and Gynaecological UnitVeena DalmeidaNo ratings yet
- AccreditationDocument17 pagesAccreditationlely.saberNo ratings yet
- Assignment: 1 Date: 12.10.2021: SolutionDocument8 pagesAssignment: 1 Date: 12.10.2021: SolutionRS BGM PRONo ratings yet
- Health MaxhxchxhnagementDocument448 pagesHealth MaxhxchxhnagementAlexandr TrotskyNo ratings yet
- The Process Variable Characteristics Variables Through Statistical MethodsDocument6 pagesThe Process Variable Characteristics Variables Through Statistical MethodsSamNo ratings yet
- Engaging Physician in Patient Safety: by - Dr. Rohit Ramesh Tiwari Dr. Sonal Sharma Ketika SikriDocument17 pagesEngaging Physician in Patient Safety: by - Dr. Rohit Ramesh Tiwari Dr. Sonal Sharma Ketika SikriRuchika RaniNo ratings yet
- Artigo 4 - Introdução Às Ferramentas de Melhoria Da Qualidade para o ClínicoDocument7 pagesArtigo 4 - Introdução Às Ferramentas de Melhoria Da Qualidade para o ClínicoLuíze FoizerNo ratings yet
- Nursing Quality Plan PDFDocument8 pagesNursing Quality Plan PDFkryztle16No ratings yet
- Lollipops For ExcellenceDocument5 pagesLollipops For ExcellenceAmR ZakiNo ratings yet
- Quality Improvement GuidlineDocument19 pagesQuality Improvement GuidlineNatnael ZemedkunNo ratings yet
- Lean Six Sigma and Quality Management in HealthcareDocument4 pagesLean Six Sigma and Quality Management in HealthcareZoya AliNo ratings yet
- 2046 4053 3 103Document6 pages2046 4053 3 103Sarat KumarNo ratings yet
- QMS-Concept Note (MERF)Document4 pagesQMS-Concept Note (MERF)mba07-807No ratings yet
- Quality Management Programs ReviewDocument5 pagesQuality Management Programs ReviewAllan SaquinNo ratings yet
- Seminar 2 Discussion QuestionDocument7 pagesSeminar 2 Discussion Questionapi-643881078No ratings yet
- 10 1 1 695 3351Document3 pages10 1 1 695 3351mahadabrata21No ratings yet
- Toolkitforbedmanagers 100531110838 Phpapp02Document84 pagesToolkitforbedmanagers 100531110838 Phpapp02RanoCenterNo ratings yet
- C11 - Basics of Quality in HSDocument6 pagesC11 - Basics of Quality in HSCoordinacion aNo ratings yet
- Qms Project #1Document16 pagesQms Project #1GirumNo ratings yet
- #12366 Electronic Medication - EditedDocument9 pages#12366 Electronic Medication - EditedNorthlandedge ConsultantsNo ratings yet
- Analysis: Adapting Lean Methods To Facilitate Stakeholder Engagement and Co-Design in HealthcareDocument4 pagesAnalysis: Adapting Lean Methods To Facilitate Stakeholder Engagement and Co-Design in HealthcareGuillermo Luis AcostaNo ratings yet
- Clinical quLITITYDocument43 pagesClinical quLITITYppniNo ratings yet
- Quality Improvement Made SimpleDocument67 pagesQuality Improvement Made Simpledan iacobNo ratings yet
- International Journal of Nursing SciencesDocument8 pagesInternational Journal of Nursing SciencesjihaanNo ratings yet
- Content ServerDocument3 pagesContent ServerShunming QiuNo ratings yet
- HSE Clinical Governance Development Matrix: June 2019Document2 pagesHSE Clinical Governance Development Matrix: June 2019SidouNo ratings yet
- Implementation PlanDocument4 pagesImplementation Planapi-557858701No ratings yet
- Quality Improvement ModelsDocument64 pagesQuality Improvement ModelsShahin Patowary100% (2)
- Bindhu Mba ProjectDocument29 pagesBindhu Mba ProjectBindu ChowdaryNo ratings yet
- Stroke Thrombectomy Mentored Implementation ProgramDocument63 pagesStroke Thrombectomy Mentored Implementation ProgramAnonymous NIPCTC68xiNo ratings yet
- A Practical Guide To Using Service User Feedback Outcome ToolsDocument99 pagesA Practical Guide To Using Service User Feedback Outcome ToolsPeter LawsonNo ratings yet
- Implementing Evidence in Clinical SettingsDocument25 pagesImplementing Evidence in Clinical SettingsDrmirfat AlkashifNo ratings yet
- Complex Interventions Guidance 29-9-08 UpdatedDocument39 pagesComplex Interventions Guidance 29-9-08 UpdatedIvan Alejandro Pulido TarquinoNo ratings yet
- Measuring quality systems in healthcare organizationsDocument13 pagesMeasuring quality systems in healthcare organizationsLaras FirdausNo ratings yet
- Quality Assurance in Mental Health and Psychiatric NursingDocument16 pagesQuality Assurance in Mental Health and Psychiatric NursingteuuuuNo ratings yet
- Is4h KCCM enDocument8 pagesIs4h KCCM enKristine De Luna TomananNo ratings yet
- 1472-6963-6-86Document11 pages1472-6963-6-86afreenahmadNo ratings yet
- The Medical Journal of AustraliaDocument5 pagesThe Medical Journal of AustraliaSyahrul YogiNo ratings yet
- Cew17111002 R2Document5 pagesCew17111002 R2Fatma HNo ratings yet
- 5 Steps To QI Final APlan Facility GuideDocument25 pages5 Steps To QI Final APlan Facility GuidejeremiahNo ratings yet
- 2020 - Quality Improvement Into PracticeDocument6 pages2020 - Quality Improvement Into PracticeMORADOMIANo ratings yet
- Quality Assurance, Obstetric Auditing, Records, Reports, Norms, Policies, Protocols, Practice and Standards For OBG UnitDocument15 pagesQuality Assurance, Obstetric Auditing, Records, Reports, Norms, Policies, Protocols, Practice and Standards For OBG UnitNileena Krishna100% (1)
- Contingency Management Approach: Implementation and OutcomesDocument112 pagesContingency Management Approach: Implementation and OutcomesArun SharmaNo ratings yet
- Using Workforce Practices To Drive Quality Improvement: A Guide For HospitalsDocument18 pagesUsing Workforce Practices To Drive Quality Improvement: A Guide For HospitalsShreeramakrishnan Ramachandran Iyer100% (1)
- Health Coaching Quality FrameworkDocument22 pagesHealth Coaching Quality FrameworkGONDHES CHANNELNo ratings yet
- Scaling Lean in Primary Care: Impacts On System Performance: ManagerialDocument10 pagesScaling Lean in Primary Care: Impacts On System Performance: ManagerialMohammad TakkoushNo ratings yet
- Quality AssuranceDocument18 pagesQuality Assurancehemihema100% (1)
- Quality Improvement Reading Material1Document10 pagesQuality Improvement Reading Material1Paul Christopher PinedaNo ratings yet
- Quality Control & Quality Improvement: Under SupervisionDocument20 pagesQuality Control & Quality Improvement: Under Supervisionheba abd elazizNo ratings yet
- Lean Into Clinical Pharmacy An Experience in ImpleDocument8 pagesLean Into Clinical Pharmacy An Experience in ImpleMildred QuispeNo ratings yet
- Eco102 Unit 8 Final Strategies For Optimal Patient CareDocument15 pagesEco102 Unit 8 Final Strategies For Optimal Patient CareAura GuzmanNo ratings yet
- Unit 1Document37 pagesUnit 1Madhu MasihNo ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationFrom EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationNo ratings yet
- Improving Sustainable Mobile Health Care Promotion - A Novel HybridDocument29 pagesImproving Sustainable Mobile Health Care Promotion - A Novel HybridojuNo ratings yet
- Disaster MGTDocument30 pagesDisaster MGTojuNo ratings yet
- Disaster 3Document28 pagesDisaster 3ojuNo ratings yet
- Disaster 2Document16 pagesDisaster 2ojuNo ratings yet
- Hybrid Mobile 4Document11 pagesHybrid Mobile 4ojuNo ratings yet
- Patient-Physician Communication: Benefits of Effective CommunicationDocument6 pagesPatient-Physician Communication: Benefits of Effective CommunicationNeneng TyasNo ratings yet
- Doctor-Patient Communication in The E-Health Era: Commentary Open AccessDocument7 pagesDoctor-Patient Communication in The E-Health Era: Commentary Open AccessojuNo ratings yet
- Communication 8Document5 pagesCommunication 8ojuNo ratings yet
- Boudreaux TBM EvaluatingSelectingMobileHealthApps 2014Document10 pagesBoudreaux TBM EvaluatingSelectingMobileHealthApps 2014ojuNo ratings yet
- ICT in EntrepreneurshipDocument5 pagesICT in EntrepreneurshipojuNo ratings yet
- Benefits of Ionic Framework App DevelopmentDocument3 pagesBenefits of Ionic Framework App DevelopmentojuNo ratings yet
- Basic Parsing TechniquesDocument34 pagesBasic Parsing TechniquesojuNo ratings yet
- Basic Parsing TechniquesDocument34 pagesBasic Parsing TechniquesojuNo ratings yet
- Using Technology To Enhance Literacy Instruction For National TransformationDocument13 pagesUsing Technology To Enhance Literacy Instruction For National TransformationojuNo ratings yet
- Fusion Accounting Hub 304046 PDFDocument14 pagesFusion Accounting Hub 304046 PDFrpgudlaNo ratings yet
- Friends or Lovers (A Novel by Rory Ridley-Duff) - View in Full Screen ModeDocument336 pagesFriends or Lovers (A Novel by Rory Ridley-Duff) - View in Full Screen ModeRory Ridley Duff92% (24)
- Bec Vantage Practice TestsDocument35 pagesBec Vantage Practice TestsHilda FlorNo ratings yet
- ClassifiedrecordsDocument23 pagesClassifiedrecordsChetana SJadigerNo ratings yet
- 122 - Motion For Leave To File Rule 11 MotionDocument3 pages122 - Motion For Leave To File Rule 11 MotionRipoff ReportNo ratings yet
- Davall Stock Gears Worm Wheel Gear Sets 17pages PDFDocument17 pagesDavall Stock Gears Worm Wheel Gear Sets 17pages PDFharish ahireNo ratings yet
- Auditing Theory - Audit ReportDocument26 pagesAuditing Theory - Audit ReportCarina Espallardo-RelucioNo ratings yet
- Personal Financial StatementDocument3 pagesPersonal Financial StatementChristopher MacLeodNo ratings yet
- Annual Report 2067 68 Final PDFDocument399 pagesAnnual Report 2067 68 Final PDFBijay Poudel100% (1)
- Llave de Impacto PDFDocument21 pagesLlave de Impacto PDFmasterfiera1No ratings yet
- JohnsonJohnson 2006 PDFDocument84 pagesJohnsonJohnson 2006 PDFakfar b417No ratings yet
- OE-254/GRC antenna parts listDocument2 pagesOE-254/GRC antenna parts listVictor GarciaNo ratings yet
- Fin4010 Assignment 3Document3 pagesFin4010 Assignment 3Grace AtteNo ratings yet
- Week 2 - Assignment SolutionsDocument2 pagesWeek 2 - Assignment SolutionsSanyamNo ratings yet
- Wagner Spring 2014 CS 161 Computer Security Midterm 1: (Last) (First)Document7 pagesWagner Spring 2014 CS 161 Computer Security Midterm 1: (Last) (First)Ahsan RamzanNo ratings yet
- Truespace For DarkBASIC ProfessionalDocument13 pagesTruespace For DarkBASIC ProfessionalclaudefrancisNo ratings yet
- Experienced Welder Seeks New OpportunityDocument2 pagesExperienced Welder Seeks New OpportunityLen HebronNo ratings yet
- Dee ChuanDocument4 pagesDee ChuanBurn-Cindy AbadNo ratings yet
- Big Kaiser2019 PDFDocument624 pagesBig Kaiser2019 PDFGoto SamNo ratings yet
- Engg Maths Sem 3 Curve FittingDocument13 pagesEngg Maths Sem 3 Curve FittingRonak Raju ParmarNo ratings yet
- LTE Data Analysis - Project Proposal N.2Document22 pagesLTE Data Analysis - Project Proposal N.2Syed SafwanNo ratings yet
- Application Form For Business Permit: Amendment: AmendmentDocument2 pagesApplication Form For Business Permit: Amendment: AmendmentJdavidNo ratings yet
- Bank Account Details and Contact NumbersDocument38 pagesBank Account Details and Contact NumbersD-Blitz StudioNo ratings yet
- Cameron VBR-II (Variable Bore Ram) PackerDocument2 pagesCameron VBR-II (Variable Bore Ram) Packerjuan olarteNo ratings yet
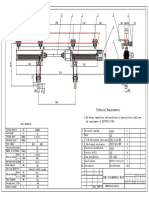
- 2X16-24 Monorail Hoist-04 - 2Document1 page2X16-24 Monorail Hoist-04 - 2RafifNo ratings yet