You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vitamins and Minerals - Vitamin ChartDocument5 pagesVitamins and Minerals - Vitamin Chartraz_939No ratings yet
- Amal HRSG-1 Project C311333 Monthly Report FormatDocument45 pagesAmal HRSG-1 Project C311333 Monthly Report FormatNadim JilaniNo ratings yet
- Bupa Insurance Letter For Couple PDFDocument1 pageBupa Insurance Letter For Couple PDFumerbutt100No ratings yet
- Garcia Rueda Vs Pascasio - DigestDocument1 pageGarcia Rueda Vs Pascasio - DigestSharon G. Balingit0% (1)
- STS Module 12 Biodiversity and The Healthy Society EnhancedDocument44 pagesSTS Module 12 Biodiversity and The Healthy Society EnhancedRyan Fernandez Dela CruzNo ratings yet
- Integrated Management of Pregnancy and ChildbirthDocument16 pagesIntegrated Management of Pregnancy and ChildbirthLea Foy-os CapiliNo ratings yet
- Diagnostic Exam 2Document5 pagesDiagnostic Exam 2Tomzki Cornelio50% (2)
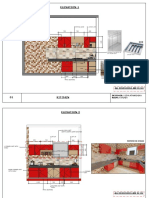
- Elevation 1: Chimney Panel L Corner UnitDocument3 pagesElevation 1: Chimney Panel L Corner UnitJeya AtharshikaNo ratings yet
- ZOning Plan of Hospital SiteDocument2 pagesZOning Plan of Hospital SiteJeya AtharshikaNo ratings yet
- PRACDocument1 pagePRACJeya AtharshikaNo ratings yet
- Submission 3Document1 pageSubmission 3Jeya AtharshikaNo ratings yet
- Next 2 PDFDocument1 pageNext 2 PDFJeya AtharshikaNo ratings yet
- Submission 1Document1 pageSubmission 1Jeya AtharshikaNo ratings yet
- Second Floor Plan: Isolation WardDocument1 pageSecond Floor Plan: Isolation WardJeya AtharshikaNo ratings yet
- Rvs School of Architecture: Rvs Educational Trust'S Group of Institutions DindigulDocument1 pageRvs School of Architecture: Rvs Educational Trust'S Group of Institutions DindigulJeya AtharshikaNo ratings yet
- First Floor PlanDocument1 pageFirst Floor PlanJeya AtharshikaNo ratings yet
- Ground FloorDocument1 pageGround FloorJeya AtharshikaNo ratings yet
- Add Model2 PDFDocument1 pageAdd Model2 PDFJeya AtharshikaNo ratings yet
- Company ProfileDocument20 pagesCompany ProfileJeya AtharshikaNo ratings yet
- Add ModelDocument1 pageAdd ModelJeya AtharshikaNo ratings yet
- 48alloy771 - Kester SDS GHS Un - English (Us)Document13 pages48alloy771 - Kester SDS GHS Un - English (Us)Joze MartinezNo ratings yet
- Patterns of Unexpected In-Hospital Deaths: A Root Cause AnalysisDocument25 pagesPatterns of Unexpected In-Hospital Deaths: A Root Cause AnalysisAmira DayoubNo ratings yet
- Hahn e Man Ns Latest PrescriptionsDocument16 pagesHahn e Man Ns Latest PrescriptionsPoonamAkhankarNo ratings yet
- Case Analysis (Kijabe Hospital) HRMDocument2 pagesCase Analysis (Kijabe Hospital) HRMMeenu GoyalNo ratings yet
- Sds Carbon Steel Welding StudDocument6 pagesSds Carbon Steel Welding StudAshley JacksonNo ratings yet
- VertigoDocument37 pagesVertigoDevi AswandiNo ratings yet
- Adult Use DispensariesDocument8 pagesAdult Use DispensariesRomeeNo ratings yet
- RA 7876 Senior Citizen CenterDocument3 pagesRA 7876 Senior Citizen CenterreadretainunderstandNo ratings yet
- Healthy Lifestyle Conversation Topics Dialogs Error Correction and S 58503Document3 pagesHealthy Lifestyle Conversation Topics Dialogs Error Correction and S 58503Luana CorrêaNo ratings yet
- Cereals: 2006 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimDocument41 pagesCereals: 2006 Wiley-Vch Verlag GMBH & Co. Kgaa, Weinheimjaime100% (1)
- 10 Best Snacks For Type 2 DiabetesDocument7 pages10 Best Snacks For Type 2 DiabetesDemuel Dee L. BertoNo ratings yet
- A Case Report On Faropenem Induced Focal SeizuresDocument3 pagesA Case Report On Faropenem Induced Focal SeizuresInternational Journal of Innovative Science and Research Technology100% (1)
- Biodata: Gabriel Ablola MD, Ma, PHD Academic and Professional QualificationsDocument1 pageBiodata: Gabriel Ablola MD, Ma, PHD Academic and Professional QualificationsboomonyouNo ratings yet
- ACE Inhibitors & Angiotensin II Antagonists: October 1997Document4 pagesACE Inhibitors & Angiotensin II Antagonists: October 1997indee533No ratings yet
- Manual Guide Kienyeji Improved PoultryDocument6 pagesManual Guide Kienyeji Improved PoultrypmbuhendwaNo ratings yet
- Care For Health-CWTSDocument15 pagesCare For Health-CWTSJAYSON BAUTISTANo ratings yet
- UEU Master 10879 Lampiran Sop - Image.markedDocument2 pagesUEU Master 10879 Lampiran Sop - Image.markedResha Noviane PutriNo ratings yet
- Nursing TheoristDocument27 pagesNursing TheoristThomas KimoloNo ratings yet
- M12FIWP12-0 - Product ManualDocument8 pagesM12FIWP12-0 - Product ManualjeanyoperNo ratings yet
- Athey, 2016Document4 pagesAthey, 2016Celeste BoxNo ratings yet
- Diabetes IN Pregnanc Y: Presenter: DR Leong Yuh Yang (MD Ukm) Supervisor: DR Noraza AzmeeraDocument45 pagesDiabetes IN Pregnanc Y: Presenter: DR Leong Yuh Yang (MD Ukm) Supervisor: DR Noraza AzmeeraKeserovic AdmirNo ratings yet
- Global Cigarette Industry PDFDocument2 pagesGlobal Cigarette Industry PDFAnkitKapoorNo ratings yet
- 24.02.09 Drawworks RepairDocument1 page24.02.09 Drawworks Repairghada gattouchNo ratings yet