You might also like
- 12lec Cardiac InfectionsDocument93 pages12lec Cardiac Infectionsmonica leeNo ratings yet
- Cardiovascular Dysfunction: (Patent Ductus Arteriosus)Document6 pagesCardiovascular Dysfunction: (Patent Ductus Arteriosus)Jc MacujaNo ratings yet
- HemorrhoidsDocument26 pagesHemorrhoidsDini Norviatin0% (1)
- Pediatric Intracranial Hypertension: Education GapDocument11 pagesPediatric Intracranial Hypertension: Education GapDiego CedamanosNo ratings yet
- Difficult Airway ManagementDocument79 pagesDifficult Airway Managementedwardjohnson2310No ratings yet
- SummonsDocument11 pagesSummonsAnthony WarrenNo ratings yet
- Congenital Heart DiseaseDocument135 pagesCongenital Heart DiseaseMahmudahNo ratings yet
- Scope and Standards of Practice For The MedicalDocument10 pagesScope and Standards of Practice For The Medicalapi-239630424100% (1)
- Case Record Book EnglishDocument31 pagesCase Record Book EnglishBabli Lovely Nicky100% (1)
- Hiv Full Report 2011Document229 pagesHiv Full Report 2011UNICEF Sverige100% (1)
- Congenital Heart Disease (CHD) : Kussia Ayano (MD)Document54 pagesCongenital Heart Disease (CHD) : Kussia Ayano (MD)Yemata HailuNo ratings yet
- CME Cyanotic Heart DiseaseDocument38 pagesCME Cyanotic Heart DiseaseTan Zhi HongNo ratings yet
- NCM209Document94 pagesNCM209Gummy BearsNo ratings yet
- Roles of Different Pharmacy Workforce (Pharmacy Supportive Personnel)Document23 pagesRoles of Different Pharmacy Workforce (Pharmacy Supportive Personnel)Tata Leizel GanzonNo ratings yet
- Case Study On Chronic Kidney Disease Probably To Secondary HypertensionDocument18 pagesCase Study On Chronic Kidney Disease Probably To Secondary Hypertensionkyeria77% (26)
- OET Writing Letter SampleDocument2 pagesOET Writing Letter Sampledrdk10% (1)
- YessDocument5 pagesYessalingh98No ratings yet
- Congenital Heart Disease (CHD)Document89 pagesCongenital Heart Disease (CHD)jefferyNo ratings yet
- Emerging Covid19 Neurology Affections. 8jul20 Supplementary-DataDocument26 pagesEmerging Covid19 Neurology Affections. 8jul20 Supplementary-DataRohan KhooshiNo ratings yet
- Coexistence of COVID-19 and Acute Ischemic Stroke Report of Four CasesDocument3 pagesCoexistence of COVID-19 and Acute Ischemic Stroke Report of Four CasessomyahNo ratings yet
- Thrombosis Research: Letter To The Editors-in-ChiefDocument3 pagesThrombosis Research: Letter To The Editors-in-ChiefRia GandaNo ratings yet
- m20 2003 PDFDocument14 pagesm20 2003 PDFTobias Ernesto Rivas GarciaNo ratings yet
- Cardiovascular Aspect of COVID-19 in Childrem Materi Prof. Najib AdvaniDocument64 pagesCardiovascular Aspect of COVID-19 in Childrem Materi Prof. Najib AdvaniJack Eugene LiowNo ratings yet
- DR Sandeep - EISENMENGER SYNDROMEDocument81 pagesDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNo ratings yet
- Jurnal CovidDocument15 pagesJurnal CovidFitriani NurFadillahNo ratings yet
- Characteristics of Ischaemic Stroke Associated With COVID-19Document3 pagesCharacteristics of Ischaemic Stroke Associated With COVID-19Qisti AshariNo ratings yet
- Congenital Heart Disease (CHD) : by Alireza PourtalebiDocument69 pagesCongenital Heart Disease (CHD) : by Alireza PourtalebiAswathy AswathyNo ratings yet
- Hypertension +++Document19 pagesHypertension +++Mohamed Tarek El KwatehyNo ratings yet
- 2021-JUN-11-phe Epi Alert Mucomycosis COVID-19 Final FDocument6 pages2021-JUN-11-phe Epi Alert Mucomycosis COVID-19 Final FNachu NachuNo ratings yet
- Clinical Pharmacology: CardiovascularDocument49 pagesClinical Pharmacology: Cardiovascularfazry 415No ratings yet
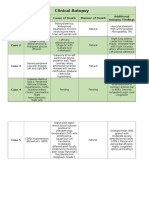
- Clinical AutopsyDocument2 pagesClinical Autopsyapi-352560644No ratings yet
- Congenital Heart Disease (CHD) : Lecture For C-I StudentsDocument89 pagesCongenital Heart Disease (CHD) : Lecture For C-I StudentsGomathi ShankarNo ratings yet
- Cha Pte R 1 1 Con Ge Nit Al Heart DiseasesDocument70 pagesCha Pte R 1 1 Con Ge Nit Al Heart DiseasessanjivdasNo ratings yet
- Narrative Review: Pulmonary Hypertension in CKDDocument11 pagesNarrative Review: Pulmonary Hypertension in CKDDr. Jatin GargNo ratings yet
- Infective Endocardits: Dr. Abhay Kumar MODERATOR-Dr. Rajesh KumarDocument42 pagesInfective Endocardits: Dr. Abhay Kumar MODERATOR-Dr. Rajesh KumarAbhay BarnwalNo ratings yet
- Cardiovasc Farmakologi Klinik0908Document49 pagesCardiovasc Farmakologi Klinik0908deka saputraNo ratings yet
- Farmakologi KardiovascularDocument49 pagesFarmakologi KardiovascularervinasetianingsihNo ratings yet
- Pulmonary HypertensionDocument27 pagesPulmonary Hypertensionantonello picernoNo ratings yet
- Delayed Acute Myocarditis and COVID 19 Relatedmultisystem in Ammatory SyndromeDocument6 pagesDelayed Acute Myocarditis and COVID 19 Relatedmultisystem in Ammatory SyndromedrKranklNo ratings yet
- 2007 Engleza Heart FailureDocument38 pages2007 Engleza Heart FailureDanielaNo ratings yet
- Acute Cardiac Failure Complicating A Case of SARS - COVID 19 in A 24-Year-Old PatientDocument2 pagesAcute Cardiac Failure Complicating A Case of SARS - COVID 19 in A 24-Year-Old PatientMedtext PublicationsNo ratings yet
- NCM 118 First SemesterDocument9 pagesNCM 118 First SemesterMutya XDNo ratings yet
- Congenital Heart DiseaseDocument12 pagesCongenital Heart DiseaseNinna Isabel VictorioNo ratings yet
- 8-Ecg in CovidsDocument35 pages8-Ecg in CovidsyandraNo ratings yet
- Prevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseaseDocument4 pagesPrevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseasenuvitaNo ratings yet
- Estado Del Arte CoronavirusDocument17 pagesEstado Del Arte CoronavirusJosé AñorgaNo ratings yet
- Approach To Patient With Dyspnea & Ankle Swellling: Dr. Mudhafar Barzani MBCHB, DM, PHD, FRCP Ass. Prof. in CardiologyDocument55 pagesApproach To Patient With Dyspnea & Ankle Swellling: Dr. Mudhafar Barzani MBCHB, DM, PHD, FRCP Ass. Prof. in CardiologyDarawan MirzaNo ratings yet
- 1 - General Assessment 2023Document12 pages1 - General Assessment 2023Mohned AlhababiNo ratings yet
- Congenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementDocument87 pagesCongenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementJZNo ratings yet
- COVID-19 Update: Covid-19-Associated Coagulopathy: Richard C. BeckerDocument14 pagesCOVID-19 Update: Covid-19-Associated Coagulopathy: Richard C. Beckersumenep nursalamNo ratings yet
- Cardiovascular and Renal Risk Factors and ComplicationsDocument16 pagesCardiovascular and Renal Risk Factors and ComplicationskajelchaNo ratings yet
- Cerebral Venous Thrombosis - Post BNT162b2 - mRNA, A Black Swan EventDocument5 pagesCerebral Venous Thrombosis - Post BNT162b2 - mRNA, A Black Swan EventLeandro L. SilvaNo ratings yet
- Bosentan Treatment For Pulmonary Arterial Hypertension Due To Patent Ductus Arteriosus and Down's Syndrome in An InfantDocument2 pagesBosentan Treatment For Pulmonary Arterial Hypertension Due To Patent Ductus Arteriosus and Down's Syndrome in An InfantOctavianus KevinNo ratings yet
- Cardiac CatheterizationDocument2 pagesCardiac CatheterizationNicola AlkhorayNo ratings yet
- Unusual Pattern of Arterial Macrothrombosis Causing Stroke in A Young Adult Recovered From COVID-19Document5 pagesUnusual Pattern of Arterial Macrothrombosis Causing Stroke in A Young Adult Recovered From COVID-19Audrey Beatrice ReyesNo ratings yet
- Covid For ClerksDocument60 pagesCovid For ClerksNehemiah FranciscoNo ratings yet
- 0717 6163 RMC 148 12 1848Document7 pages0717 6163 RMC 148 12 1848ViondaA SotoNo ratings yet
- Venous Thromboembolism DiseaseDocument49 pagesVenous Thromboembolism DiseaseNiko YuandikaNo ratings yet
- 2020 Article 2134Document14 pages2020 Article 2134Maysa HasanahNo ratings yet
- Congenital Heart Diseases: Prof. Dr. Md. Nazrul IslamDocument23 pagesCongenital Heart Diseases: Prof. Dr. Md. Nazrul IslamprajwalNo ratings yet
- The Spectrum of Cardiac Manifestations in Coronavirus Disease 2019 (COVID-19) - A Systematic Echocardiographic StudDocument31 pagesThe Spectrum of Cardiac Manifestations in Coronavirus Disease 2019 (COVID-19) - A Systematic Echocardiographic StudsamuelNo ratings yet
- Hypertension FinalDocument24 pagesHypertension FinalFlorencio D. Santos IVNo ratings yet
- The Spectrum of Cardiac Manifestations in Coronavirus Disease 2019 (COVID-19) - A Systematic Echocardiographic StudyDocument31 pagesThe Spectrum of Cardiac Manifestations in Coronavirus Disease 2019 (COVID-19) - A Systematic Echocardiographic Studyre septian IlhamsyahNo ratings yet
- CHN Midterm CoverageDocument15 pagesCHN Midterm CoverageMaria Theresa BuscasNo ratings yet
- FINALS ch31Document6 pagesFINALS ch31Monica JubaneNo ratings yet
- Considerations For Heart Failure Care During The COVID-19 PandemicDocument11 pagesConsiderations For Heart Failure Care During The COVID-19 PandemicBasilio BabarNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- New-Infective EndocarditisDocument30 pagesNew-Infective Endocarditisزياد سعيدNo ratings yet
- Innovative Physiotherapy Clinical Education in Response To The COVID-19 Pandemic With A Clinical Research Placement ModelDocument3 pagesInnovative Physiotherapy Clinical Education in Response To The COVID-19 Pandemic With A Clinical Research Placement ModelGeysel SuarezNo ratings yet
- Accepted Manuscript: 10.1016/j.jevs.2017.10.013Document27 pagesAccepted Manuscript: 10.1016/j.jevs.2017.10.013Geysel SuarezNo ratings yet
- Annals of Medicine and Surgery: Sara Bouabdella, Soraya Aouali, Hanan Ragragui, Nada Zizi, Siham DikhayeDocument3 pagesAnnals of Medicine and Surgery: Sara Bouabdella, Soraya Aouali, Hanan Ragragui, Nada Zizi, Siham DikhayeGeysel SuarezNo ratings yet
- N 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CDocument18 pagesN 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CGeysel SuarezNo ratings yet
- Annals of Medicine and Surgery: Motohiro Kikukawa, MD, Akira Kuriyama, MD, DRPH, PHDDocument3 pagesAnnals of Medicine and Surgery: Motohiro Kikukawa, MD, Akira Kuriyama, MD, DRPH, PHDGeysel SuarezNo ratings yet
- Annals of Medicine and Surgery: Bareza Rezaei, Elahe Mousavi, Bahram Heshmati, Shaphagh AsadiDocument8 pagesAnnals of Medicine and Surgery: Bareza Rezaei, Elahe Mousavi, Bahram Heshmati, Shaphagh AsadiGeysel SuarezNo ratings yet
- Quadriceps Strength Is A Sensitive Marker of Disease Progression in Sporadic Inclusion Body MyositisDocument7 pagesQuadriceps Strength Is A Sensitive Marker of Disease Progression in Sporadic Inclusion Body MyositisGeysel SuarezNo ratings yet
- Laban 1995Document4 pagesLaban 1995Geysel SuarezNo ratings yet
- Research in Developmental DisabilitiesDocument7 pagesResearch in Developmental DisabilitiesGeysel SuarezNo ratings yet
- 10.1016@S2171 97480870037 0Document5 pages10.1016@S2171 97480870037 0Geysel SuarezNo ratings yet
- Maisuradze 2012Document16 pagesMaisuradze 2012Geysel SuarezNo ratings yet
- Herniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryDocument6 pagesHerniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryGeysel SuarezNo ratings yet
- Clinical Neurophysiology: Erdal Binbog A, Kemal S. TürkerDocument8 pagesClinical Neurophysiology: Erdal Binbog A, Kemal S. TürkerGeysel SuarezNo ratings yet
- Forsberg 2005Document11 pagesForsberg 2005Geysel SuarezNo ratings yet
- Jocs 14583Document4 pagesJocs 14583Geysel SuarezNo ratings yet
- COVID-19 in Kidney Transplant Recipients: Original ArticleDocument7 pagesCOVID-19 in Kidney Transplant Recipients: Original ArticleGeysel SuarezNo ratings yet
- Invasive Mechanical Ventilation in COVID-19 Patient Management: The Experience With 469 Patients in WuhanDocument3 pagesInvasive Mechanical Ventilation in COVID-19 Patient Management: The Experience With 469 Patients in WuhanGeysel SuarezNo ratings yet
- Guillain-Barre Syndrome Patient's Satisfaction With Physiotherapy: A Two-Part Observational StudyDocument8 pagesGuillain-Barre Syndrome Patient's Satisfaction With Physiotherapy: A Two-Part Observational StudyGeysel SuarezNo ratings yet
- Treatment of Coronavirus Disease 2019 (COVID-19) Patients With Convalescent PlasmaDocument11 pagesTreatment of Coronavirus Disease 2019 (COVID-19) Patients With Convalescent PlasmaGeysel SuarezNo ratings yet
- Safety and Health at Work: Kyung-Sun Lee, Myung-Chul JungDocument9 pagesSafety and Health at Work: Kyung-Sun Lee, Myung-Chul JungGeysel SuarezNo ratings yet
- Nguyen 2001Document5 pagesNguyen 2001Geysel SuarezNo ratings yet
- Miller Fisher Syndrome and Guillain-Barré Syndrome: Dual Intervention Rehabilitation of A Complex Patient CaseDocument11 pagesMiller Fisher Syndrome and Guillain-Barré Syndrome: Dual Intervention Rehabilitation of A Complex Patient CaseGeysel SuarezNo ratings yet
- Focused Reviews: Barriers and Strategies For Early Mobilization of Patients in Intensive Care UnitsDocument7 pagesFocused Reviews: Barriers and Strategies For Early Mobilization of Patients in Intensive Care UnitsGeysel SuarezNo ratings yet
- Office Technology and People: Article InformationDocument19 pagesOffice Technology and People: Article InformationGeysel SuarezNo ratings yet
- Physical Training Injuries and Interventions For Military RecruitsDocument6 pagesPhysical Training Injuries and Interventions For Military RecruitsGeysel SuarezNo ratings yet
- Kirkeby Garstad2005Document7 pagesKirkeby Garstad2005Geysel SuarezNo ratings yet
- Causes of Sterile Pyuria Infection RelatedDocument2 pagesCauses of Sterile Pyuria Infection RelatedSarah AhmedNo ratings yet
- 1 - Indocyanine Green-Enhanced Fluorescence To Assess BowelDocument7 pages1 - Indocyanine Green-Enhanced Fluorescence To Assess BowelIcaro DanielNo ratings yet
- Triase IGD Maret 2021Document33 pagesTriase IGD Maret 2021IRAYANANo ratings yet
- RewtrewyewtewDocument9 pagesRewtrewyewtewNom NomNo ratings yet
- ERAS Perioperative Care in Lumbar Spine FusionDocument24 pagesERAS Perioperative Care in Lumbar Spine FusionDionisius RiantoNo ratings yet
- Subjective Examination Template 2022Document5 pagesSubjective Examination Template 2022LibbyNo ratings yet
- International Society For Technology in Arthroplasty - Indicação de ArtigosDocument77 pagesInternational Society For Technology in Arthroplasty - Indicação de ArtigosJosé santanaNo ratings yet
- Susruthasamhitha Part 3Document42 pagesSusruthasamhitha Part 3Suvarna NalapatNo ratings yet
- Ricardo Padilla Perez v. Secretary of Health & Human Services, 985 F.2d 552, 1st Cir. (1993)Document10 pagesRicardo Padilla Perez v. Secretary of Health & Human Services, 985 F.2d 552, 1st Cir. (1993)Scribd Government DocsNo ratings yet
- Zestlife Dental Cover Brochure 2023 No Core IndvDocument10 pagesZestlife Dental Cover Brochure 2023 No Core IndvJames FrankoNo ratings yet
- Fridays LawsDocument2 pagesFridays LawsAHRMMNo ratings yet
- Patient Profile Patient Address Age Sex MaritalDocument3 pagesPatient Profile Patient Address Age Sex Maritalunno hiquianaNo ratings yet
- Psychotherapeutic AgentsDocument2 pagesPsychotherapeutic AgentsjustinahorroNo ratings yet
- Anterior Cranial Base Timerelated Changes A Systematic Review PDFDocument18 pagesAnterior Cranial Base Timerelated Changes A Systematic Review PDFNataly ComettaNo ratings yet
- Bolgan DR - Ssa Loretta-Meccanismo D'induzione Del Danno Da Vaccini A mRNADocument34 pagesBolgan DR - Ssa Loretta-Meccanismo D'induzione Del Danno Da Vaccini A mRNAgiordana214No ratings yet
- Psychosis in WomenDocument7 pagesPsychosis in WomenMarius PaţaNo ratings yet
- Spain Visa Application CenterDocument2 pagesSpain Visa Application CenterMansoor AliNo ratings yet
- A Guide: Christian Medical CollegeDocument75 pagesA Guide: Christian Medical CollegeSanjay Kumar SekhardeoNo ratings yet
- Reiman Et Al 2017 Cannabis As A Substitute For Opioid Based Pain Medication Patient Self ReportDocument7 pagesReiman Et Al 2017 Cannabis As A Substitute For Opioid Based Pain Medication Patient Self ReportfelipepretelmktNo ratings yet