Professional Documents
Culture Documents
Conceptualizations of Clinical Leadership: A Review of The Literature
Uploaded by
Bayu PrabuOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Conceptualizations of Clinical Leadership: A Review of The Literature
Uploaded by
Bayu PrabuCopyright:
Available Formats
Journal of Healthcare Leadership Dovepress
open access to scientific and medical research
Open Access Full Text Article REVIEW
Conceptualizations of clinical leadership: a review
of the literature
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
This article was published in the following Dove Press journal:
Journal of Healthcare Leadership
27 October 2017
Number of times this article has been viewed
Solange Mianda Introduction: Poor patient outcomes in South African maternal health settings have been
Anna S Voce associated with inadequately performing health care providers and poor clinical leadership at the
point of care. While skill deficiencies among health care providers have been largely addressed,
Department of Public Health
Medicine, School of Nursing and the provision of clinical leadership has been neglected. In order to develop and implement initia-
Public Health, College of Health tives to ensure clinical leadership among frontline health care providers, a need was identified
For personal use only.
Sciences, University of KwaZulu-
Natal, Durban, South Africa
to understand the ways in which clinical leadership is conceptualized in the literature.
Design: Using the systematic quantitative literature review, papers published between 2004 and
2016 were obtained from search engines (Google Scholar and EBSCOhost). Electronic databases
(CINHAL, PubMed, Medline, Academic Search Complete, Health Source: Consumer, Health
Source: Nursing/Academic, ScienceDirect and Ovid®) and electronic journals (Contemporary
Nurse, Journal of Research in Nursing, Australian Journal of Nursing and Midwifery, Interna-
tional Journal of Clinical Leadership) were also searched.
Results: Using preselected inclusion criteria, 7256 citations were identified. After screening
230 potentially relevant full-text papers for eligibility, 222 papers were excluded because they
explored health care leadership or clinical leadership among health care providers other than
frontline health care providers. Eight papers met the inclusion criteria for the review. Most
studies were conducted in high-income settings. Conceptualizations of clinical leadership share
similarities with the conceptualizations of service leadership but differ in focus, with the intent
of improving direct patient care. Clinical leadership can be a shared responsibility, performed by
every competent frontline health care provider, regardless of the position in the health care system.
Conclusion: Conceptualizations of clinical leadership among frontline health care providers
arise mainly from high-income settings. Understanding the influence of context on conceptual-
izations of clinical leadership in middle- and low-income settings may be required.
Keywords: clinical leadership, conceptualizations, frontline health care providers
Introduction
Clinical leadership plays a key role in ensuring both quality patient care and creating
a healthy and safe clinical work environment.1–3 Poor patient care and adverse events
have been reported in health facilities around the world, prompting health systems to
call for strong clinical leadership.1–3
Correspondence: Solange Mianda
Department of Public Health Medicine, In South Africa, in maternal health settings, poor care has been associated with
School of Nursing and Public Health, inadequate competencies among health care providers and poor clinical leadership,4,5
College of Health Sciences, University
of KwaZulu-Natal, Room 236, Second resulting in recommendations emphasizing the need to improve clinical skills and to
Floor George Campbell Building, Durban, improve clinical mentoring and clinical leadership.2,4,5 While programs to develop
South Africa
Tel +27 84 279 4310 clinical skills, particularly lifesaving skills, have been rolled out actively,6,7 less atten-
Email solange.zoe60@gmail.com tion has been paid to the provision of clinical leadership.
submit your manuscript | www.dovepress.com Journal of Healthcare Leadership 2017:9 79–87 79
Dovepress © 2017 Mianda and Voce. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.
http://dx.doi.org/10.2147/JHL.S143639
php and incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing the work
you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For
permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms (https://www.dovepress.com/terms.php).
Powered by TCPDF (www.tcpdf.org)
Mianda and Voce Dovepress
Initiatives to promote and develop clinical leadership ursing, Australian Journal of Nursing and Midwifery, Inter-
N
among frontline health care providers have been implemented national Journal of Clinical Leadership) were searched. The
in the UK, the USA, Canada and Australia. However, in search was limited to articles published between 2004 and
Africa generally and in South Africa specifically, there has 2016, to ensure the most recent published literature would be
been slow progress in promoting and developing clinical obtained through the review. The search terms included “clin-
leadership among frontline health care providers,8 with ical leadership” in combination with: “conceptualization”,
the concepts of clinical leadership and clinical leadership “characteristics”, “definition”, “medical”, “perceptions”,
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
development still underresearched.8 Furthermore, the lit- “perspectives” and “roles”; and “frontline leadership” in
erature on leadership in the health sector focuses mostly on combination with: “nursing”, “perceptions”, “perspectives”,
health service leadership rather than on clinical leadership “roles”, “characteristics”, “conceptualization” and “defini-
of frontline health care providers.9 tion”. The reference sections of accessed articles were also
Frontline health care providers, for example, nurses, consulted to ensure the review was comprehensive.
midwives, allied health care providers and doctors providing Research papers were considered for inclusion in the
direct patient care, are well positioned for providing, and review if they met the following criteria: 1) original research
benefiting from, the clinical leadership required to ensure paper published in a peer-reviewed journal; 2) gray literature;
both quality patient care and a healthy and safe clinical work 3) exploring definitions/conceptualizations/perceptions of
environment.1,10–12 However, in many cases, frontline health clinical leadership; 4) from the perspectives of frontline health
care providers are neither clear about what is clinical leader- care providers; and 5) published in the English language. Stud-
For personal use only.
ship nor are well prepared to provide it.2,13,14 Moreover, front- ies that did not explore clinical leadership among frontline
line health care providers do not have clear career pathways health care providers, studies that explored health care leader-
to encourage them to engage in clinical leadership roles.9 ship, literature reviews and systematic reviews were excluded.
Toward describing what is clinical leadership among
frontline health care providers, a literature review was con- Assessing publications
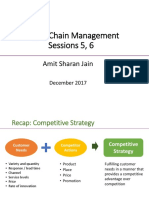
ducted as part of a doctoral research project. The overall aim The literature search resulted in 7256 citations. Figure 1
of the doctoral project was to develop a model of clinical presents the study flow mapping out the number of records
leadership among frontline health care providers in labor identified, included and excluded and the reasons for their
wards of district hospitals in KwaZulu-Natal, South Africa. exclusion. After screening 230 potentially relevant full-text
papers for eligibility, 183 papers were excluded because they
Aim explored health care leadership and 39 papers were excluded
The aim of the literature review was to establish from pub- for not exploring clinical leadership among frontline health
lished literature how clinical leadership is conceptualized, care providers or being literature reviews. Eight papers met
from the perspective of frontline health care providers. the inclusion criteria and were analyzed for the review.
The quality of studies reviewed was appraised using the
Design most appropriate tool. The “strengthening the reporting of
The systematic quantitative literature review method15 was observational studies in epidemiology” (STROBE),16 the
followed to search and identify relevant literature and to “consolidated criteria for reporting qualitative research”
extract conceptualizations of clinical leadership among (COREQ) 17 and the “mixed methods appraisal tool”
frontline health care providers. Published literature was (MMAT)18 were used for the appraisal. Against the STROBE
reviewed and guided by the question: “How is clinical leader- criteria, the articles reporting the results of the quantitative
ship conceptualized among frontline health care providers”? studies did not provide clear descriptions of study designs.
However, they included sound descriptions of variables, data
Search method collection methods and data analysis. Against the COREQ
The search started within large search engines (Google criteria, the qualitative studies contained several shortcom-
Scholar and EBSCOhost). The search extended to electronic ings, particularly related to the implementation of critical
databases (CINHAL, PubMed, Medline, Academic Search reflexivity19,20 and the relationship between researchers and
Complete, Health Source: Consumer, Health Source: Nurs- participants. Furthermore, poor alignment was observed
ing/Academic, ScienceDirect and Ovid®). Lastly, electronic between the reported methodological orientation under-
journals (Contemporary Nurse, Journal of Research in pinning the studies and the data collection and analysis
80 submit your manuscript | www.dovepress.com Journal of Healthcare Leadership 2017:9
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Conceptualizations of clinical leadership
Records identified through Additional records
database searching identified through other
(n=7251) sources
(n=5)
Records excluded
Records screened -Duplicate
(n=7256) -Not relevant to clinical
leadership
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
n=7026
Records assessed for Records excluded
eligibility -Health care leadership
(n=230) (n=183)
Full-text articles excluded, with
Full-text articles assessed reasons
for eligibility
-Literature reviews
(n=47)
-Clinical leadership among other
professionals
(n=39)
For personal use only.
Studies included in
qualitative synthesis
(n=8)
Figure 1 Study flow mapping out the number of records identified, included and excluded and the reasons for their exclusion.
methods. Against the MMAT criteria, although the rationale method section for the literature review was drafted. Finally,
for integrating quantitative and qualitative methods was articles included were thematically analyzed to establish
explained, there was neither clear indication of the process conceptualizations of clinical leadership among frontline
implemented for the integration of data nor clear indication health care providers.
of the limitations associated with the integration. Overall,
studies used appropriate methodological approaches. Two Results
studies, one qualitative and the other quantitative, utilized A total of eight papers published between 2004 and 2016 were
research designs with sufficient strength to produce transfer- included in this review. Table 1 presents the characteristics
able and generalizable findings.21,22 The deficiencies identified of identified studies.
in different studies did not detract from the purpose of this
literature review. Study settings
Three papers report on studies conducted in Australia,19,23,24
Constructing the database three in the UK,20,21,25 one in Ireland14 and one study con-
From each paper exploring conceptualizations of clinical ducted in New Zealand.22
leadership, the following information was recorded in a
database: setting where the study was conducted; study aim, Aims of the studies
study design, study population and sample size; the clinical All eight studies were designed to identify, explore, inves-
field in which the studies were conducted and conceptualiza- tigate, describe or capture the views of frontline health care
tions of clinical leadership. providers on the concept of clinical leadership.
Recording data in the database Study design
Papers were recorded in the database to check whether the The papers included in the review reported on the implemen-
categories created assisted to capture relevant data. No cor- tation of a diversity of study designs: qualitative, quantitative
rections were needed with the categories identified. The and mixed method designs were used.
Journal of Healthcare Leadership 2017:9 submit your manuscript | www.dovepress.com
81
Dovepress
Powered by TCPDF (www.tcpdf.org)
Mianda and Voce Dovepress
Table 1 Characteristics of identified studies
Study Study aim Study design Study Clinical Key findings – clinical leadership
setting population field conceptualized as
and author and sample
(year) size
Australia; Identify Study design: sequential mixed method Ambulance Ambulance - the qualities and competence of
Stanley et al how clinical using: literature review and expert service staff services leaders (caring, moral values, skill and
(2013)23 leadership review to inform questionnaire design, – 250 experience ability to promote change,
is perceived quantitative descriptive survey and ability to impact on standards of care)
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
based on the qualitative descriptive survey - having the resources necessary to
experiences Data collection: document reviews, perform tasks effectively
of ambulance self-administered questionnaires and
service staff individual in-depth interviews
Data analysis: thematic analysis to
develop questionnaire, descriptive
statistics for characteristics of clinical
leaders and thematic analysis for
conceptualizations of clinical leadership
Australia; Identify how Study design: quantitative descriptive Allied health Allied health - the qualities and competence of
Stanley et al the concept survey professionals professions leaders (communication, clinical
(2017)24 of clinical Data collection method: self- – 307 competence, approachability, setting
leadership is administered, closed questions with direction, role model)
For personal use only.
perceived by open options - a responsibility/role for everyone
allied health Data analysis: descriptive statistics and and not located at specific levels
professionals content analysis within the health system
Australia; Explore the Study design: grounded theory Nurses – 12 Mental - the qualities and competence
Ennis et al perceptions of Data collection method: semi- health of leaders (ability to remain calm
(2015)19 nurses of what structured and individual interviews and confident in time of crisis and
constitutes Data analysis: constant comparative uncertainty, manage unpredictable
effective analysis situations)
clinical
leadership
UK; Burns Explore the Study design: descriptive General Nursing - the qualities and competence of
(2009)21 concept phenomenology practice leaders (being there; available to
of clinical Data collection method: in-depth nurses – 12 support, advise, encourage and guide
leadership individual interviews as necessary; understanding of the
Data analysis: descriptive role of clinical leadership to provide
phenomenology support as required)
UK; British Explore Study design: not specified Doctors (GPs, - the qualities and competence of
Medical perspectives Data collection method: focus group consultants, leaders (role modeling, provide vision,
Association of medical discussions and semi-structured staff grade, able to gain support and influence
(2012)25 doctors questionnaires specialty others, demonstrate expertise)
on clinical Data analysis: not specified (probably doctors, - being clinically engaged
leadership thematic analysis) associate - distinct from (health service)
specialists) management
– 70
UK; Mendis Explore Study design: sequential mixed Trainee Medicine - the qualities and competence
and Paton opinions methods; literature review to inform registrars – of leaders (reflective practice,
(2014)20 on clinical questionnaire design, quantitative 247 moral values, do no harm, good
leadership descriptive survey and qualitative communication skills, role model,
descriptive survey competence, clinical decision-making,
Data collection: self-administered acting in the patient best interest)
questionnaires with multiple answer - important in promoting
options and individual semi-structured professionalism and teamwork
interviews with open-ended options - delivering change in patient care
Data analysis: descriptive statistics and
thematic analysis
(Continued)
82 submit your manuscript | www.dovepress.com Journal of Healthcare Leadership 2017:9
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Conceptualizations of clinical leadership
Table 1 (Continued)
Study Study aim Study design Study Clinical Key findings – clinical leadership
setting population field conceptualized as
and author and sample
(year) size
Ireland; Describe Study design: not specified Nurses – 144 Nursing and - the qualities and competence of
McNamara views of Data collection method: focus group midwifery leaders (influencing and motivating
et al (2011)14 clinical discussions using topic guide others to deliver effective patient
leadership Data analysis: thematic analysis care, requiring practical expertise)
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
- representing the nursing
contribution to care
- effective teamwork
New Zealand; Explore the Study design: quantitative, descriptive Registered Mental - the qualities and competence of
Trimmer perception and comparative nurses – 21 health leaders (role model, mentor, assess
(2007)22 of clinical Data collection: self-administered performance, communicate)
leadership closed questions with open options - related to staff retention
distributed via mail - improving patient outcomes
Data analysis: descriptive, comparative - related to organizational support
statistics and thematic analysis of open - continued medical education
questionnaire
Abbreviation: GP, general practitioner.
For personal use only.
Grounded theory and phenomenology were used induc- in the quantitative studies. The response rates of survey ques-
tively to generate conceptualizations of clinical leadership tionnaires ranged between 6.1% and 56.0%. The sample sizes
from the experiences of frontline health care providers. Con- enrolled in the identified studies ranged from small numbers
stant comparative analysis and thematic analysis contributed (n=12) in the qualitative studies to relatively large numbers
to identifying key domains of clinical leadership from the in the survey-based designs (n=307).
perspectives of frontline health care providers.
Deductive quantitative designs were used to test the level Clinical field in which the studies were
of agreement with variables contained in existing frame- conducted
works describing clinical leadership. Based on the scoring Conceptualizations of clinical leadership were explored from
of descriptive statements, conceptualizations of clinical the perspective of frontline health care providers in mental
leadership were advanced. health, medical practice, nursing and midwifery, ambulance
Sequential mixed methods design used literature reviews, services and residential facilities. Allied health profession-
expert reviews and in-depth interviews to inform question- als’ perspectives on clinical leadership were also explored.
naire design to advance descriptions of clinical leadership,
with which respondents could indicate the level of agreement. Conceptualizations of clinical
Study population and sampling strategies leadership
Conceptualizations of clinical leadership as gleaned from
Studies comprised frontline health care providers (nurses,
the studies included in the review can be grouped into six
midwives, ambulance personnel, allied health professionals
distinctive broad themes:
and doctors from different specialties).
Purposive sampling was used in the qualitative studies 1. Clinical leadership conceptualized as having a focus on
to select participants. Homogeneous sampling was used to patient care: clinical leadership was conceptualized as
capture the perspectives of clinical leadership from a par- having a focus on direct patient care.14,20,22
ticular perspective, for example, nurses, midwives, allied 2. Clinical leadership conceptualized as purpose: clinical
health professionals or ambulance personnel. Heterogeneous leadership was conceptualized as having the purpose
sampling was used to elicit multiple perspectives on clinical of delivering change in the quality of direct patient care
leadership, for example, doctors from different specialties. and, furthermore, to motivate members of the team to
Online surveys, training programs, student databases and provide effective health care that is safe and satisfying to
health service provision sites were used to recruit participants patients. Clinical leadership was also perceived as having
Journal of Healthcare Leadership 2017:9 submit your manuscript | www.dovepress.com
83
Dovepress
Powered by TCPDF (www.tcpdf.org)
Mianda and Voce Dovepress
the purpose of promoting staff retention and providing Thus, t ransferability of findings from this literature review to
organizational support, in the effort to improve patient clinical leadership among frontline health care providers in
outcomes.14,20,23 South African labor wards might be compromised. Original
3. Clinical leadership conceptualized as the qualities of research focusing on conceptualizations of clinical leadership
clinical leaders: clinical leadership was conceptualized in low-and middle-income settings, including South Africa,
as the qualities and competencies of clinical leaders. is recommended for understanding contextual influences on
Qualities attributed to effective clinical leaders include conceptualizations of clinical leadership among frontline
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
approachability, role modeling, visibility and availability health care providers.
to support, advise and guide, capacity to remain calm and Conceptualizations of clinical leadership uncovered in
confident in crisis, ability to gain support and influence this review were thematically depicted as purpose, as quali-
others, ability to promote change, ability to communicate ties of leaders, as competence of leaders, as a set of roles to
effectively and impact on standards of care.14,19–23,25 be performed and as a position of authority. The thematic
4. Clinical leadership conceptualized as the competencies of depictions of clinical leadership may not be conceptually
clinical leaders: clinical leaders’ competencies included distinct from conceptualizations of health services leader-
demonstrating clinical expertise; being clinically focused, ship.26 Clinical leadership and health service leadership
remaining clinically engaged, understanding clinical may indeed be similarly conceptualized and share charac-
leadership roles and clinical decision making.14,19–23,25 teristics.3,26 However, a different focus may be evident, with
5. Clinical leadership conceptualized as roles: clinical clinical leadership focusing on direct patient care14,21,22 and
For personal use only.
leadership was conceptualized as a role to be fulfilled health service leadership focusing on providing a supportive
by every frontline health care provider, regardless of the context (policy, strategy and resource allocation), within
position in the health system. Clinical leadership roles which effective clinical leadership and optimal patient care
identified included setting direction, providing the vision may be exercised.3,26
and promoting professionalism, teamwork, interprofes- Clinical leadership is distinct from health service manage-
sional collaborations, good practice and continued medi- ment.19,20,24,25 In clinical settings, clinical decisions are made
cal education. Clinical leadership was also perceived as by frontline health care providers within clinical teams.2,27,28
representing the nursing contribution to patient care and Frontline health care providers exercise their leadership roles
having the resources to perform tasks effectively.14,22,23 in health service management through expert power, by virtue
6. Clinical leadership conceptualized as distinct from health of their training and specialist knowledge, rather than through
service management: clinical leadership was not linked a position in the management hierarchy.27,29
to a position held within the management structure and Clinical leadership was conceptualized as a role to be
hierarchy of the organization.19,20,24,25 performed by every frontline health care provider in direct
contact with patients, regardless of the position held in the
Discussion organizational hierarchy.14,21,22,27 Shared clinical leadership
This review was conducted to explore conceptualizations of models depart from traditional leadership models in that
clinical leadership in the literature, from the perspectives of leadership is distributed among individuals instead of being
frontline health care providers. Eight papers met the inclusion embodied in one individual.28,30 Shared clinical leadership
criteria. The papers were reviewed for quality and content, promotes teamwork, where each team member’s skills and
and conceptualizations of clinical leadership were summa- experiences are valued and used to attain optimal patient
rized and synthesized. outcomes.28,30 Shared clinical leadership relies on human rela-
All eight papers included in the review reflect studies tions, influence and democracy, within flatter organizational
conducted in high-income settings. Although health sys- structures.27,28 The challenges with shared clinical leadership,
tems around the world share basic similar structures, the however, might be how to adopt models of shared clinical
context in which clinical leadership is exercised might differ leadership in predominantly hierarchical organizational
between high-income and low- and middle-income settings. structures.28,31 In emergency situations when rapid decisions
Low- and middle-income settings generally suffer from are required, the democratic nature of decision making in
underresourced and poorly managed health systems,8 which shared leadership might not allow sufficient consultation
might challenge clinical leadership and the ways in which it with everyone involved.28,31 Shared clinical leadership may
is conceptualized and experienced by health care providers. be thwarted in clinical settings where professional power
84 submit your manuscript | www.dovepress.com Journal of Healthcare Leadership 2017:9
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Conceptualizations of clinical leadership
differentials exist, for example, in doctor-led services, where Limitations of the study
nurses and midwives may be reticent to make clinical deci- Although rigorous steps were followed in this review, we are
sions they indeed are empowered to make.32,33 also aware of some limitations.
The purpose of clinical leadership appears to be influ-
• First, studies may have been omitted from the review if
enced by a service orientation,14,21–23,34 primarily service to
they were not published in the databases searched or if
patients and secondarily to staff, but for the sake of optimal
they were published in languages other than English.
patient care.11
• Second, the decision to limit the search to articles that
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
Frontline health care providers conceptualized clinical
reported conceptualizations of clinical leadership among
leadership as a set of roles, highlighting the roles of the leader
“frontline health care providers” reduced the range of
as visionary, as a role model and as an expert, coach and men-
articles included in the review.
tor that contribute to building excellence and interpersonal
trust and teamwork.14,21–23
Conceptualizations of clinical leadership, which fore-
Conclusion
Frontline health care providers through this review con-
grounded the qualities and competencies of clinical lead-
ceptualized clinical leadership as purpose, qualities and
ers, may be influenced by trait and behavioral leadership
competence of leaders, as a set of roles to be performed and
theories.14,19,20,23,24,26 However, a particular emphasis seems
as a position held in the organizational hierarchy. Frontline
to have been placed on the actual clinical expertise of the
health care providers conceptualized clinical leadership as
clinical leader.22,25 This suggests that fundamental to the
For personal use only.
being distinct from health service leadership, with a direct
provision of clinical leadership is clinical competence. Clini-
patient care focus requiring highly clinically competent
cal competence is required to build the clinical skills and
frontline health care providers to produce optimal patient
expertise of the individual and team and to lift standards of
care. Clinical leadership roles may be shared among front-
patient care.23 Approaches to building clinical competence
line health care providers, regardless of the position held
can incorporate principles of shared leadership in an orga-
in the organizational hierarchy, to ensure positive patient
nizational culture of cooperation toward the attainment of
outcomes. However, shared clinical leadership works best in
optimal patient care.28,35
flatter organizational structures and nonhierarchical patterns
Conceptualizations of clinical leadership from the per-
of human relationships. Strong hierarchical organizational
spective of frontline health care providers were extracted
structures and ways of relating may present a challenge to
from the literature, identifying key features of clinical lead-
the implementation of shared clinical leadership in clinical
ership. However, what does not transpire from the literature
settings. Further research to explore the influence of context
is how the conceptual characteristics of clinical leadership
and organizational structure on conceptualizations of clinical
are implemented in the clinical setting. Hence, one potential
leadership may be required.
research agenda is to conduct a primary study to establish
how different conceptual characteristics of clinical leader-
ship are connected to optimal patient care. Furthermore, Acknowledgments
the body of published works on clinical leadership from the Special thanks go to D. Stanley (Professor of Nursing, Uni-
perspective of frontline health care providers is limited and versity of New England, Western New South Wales) for his
therefore does not permit comparisons of conceptualiza- comments on the draft of this article. This paper is part of a
tions among different clinical professions. A primary study doctoral study partly funded through a scholarship from the
to explore profession-specific conceptualizations may well College of Health Sciences at the University of KwaZulu-
be indicated. Natal. This review used secondary data from several data-
bases available to the public. Except for the data presented
Strengths of the study in this study, there is no additional data for sharing.
This review highlights the diversity, extent and gaps of the
research on the conceptualizations of clinical leadership Author contributions
among frontline health care providers. Further, the review SM (University of KwaZulu-Natal) was the project leader
has identified key directions for further research on concep- involved throughout the study processes, from project design
tualizations of clinical leadership. to write-up.
Journal of Healthcare Leadership 2017:9 submit your manuscript | www.dovepress.com
85
Dovepress
Powered by TCPDF (www.tcpdf.org)
Mianda and Voce Dovepress
AV (University of KwaZulu-Natal) is the first author’s PhD 16. Vandenbroucke J, von Elm E, Altman DG, et al. Strengthening the
Reporting of Observational Studies in Epidemiology (STROBE): expla-
supervisor who made conceptual contributions and provided nation and elaboration. Ann Intern Med. 2007;147(8):W163–W194.
technical guidance throughout the writing processes (revising 17. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualita-
the article and approval of the final version for submission). tive research (COREQ): a 32-item checklist for interviews and focus
groups. Int J Qual Health Care. 2007;19(6):349–357.
All authors contributed to data analysis, drafting and 18. Pluye P, Hong QN [webpage on the Internet]. Appraising qualitative,
revising the paper and agree to be accantable for all aspect quantitative, and mixed methods studies included in mixed studies reviews:
the MMAT. Annu Rev Public Health. 2011. Available from: http://mixed-
of the work. methodsappraisaltoolpublic.pbworks.com. Accessed June 8, 2017.
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
19. Ennis G, Happell B, Reid-Searl K. Enabling professional development
Disclosure in mental health nursing: the role of clinical leadership. J Psychiatr
Ment Health Nurs. 2015;22(8):616–622.
The authors report no conflicts of interest in this work. 20. Mendis D, Paton C. Perceptions of clinical leadership amongst West
Midlands registrars. Int J Leadersh Public Serv. 2014;10(2):108–122.
21. Burns D. Clinical leadership for general practice nurses, part 1: per-
References ceived needs. Pract Nurs. 2009;20(9):466–469.
1. Daly J, Jackson D, Mannix J, Davidson P, Hutchinson M. The impor- 22. Trimmer W. The Way Things Are Done Around Here: Perceptions of
tance of clinical leadership in the hospital setting. J Healthc Leadersh. Clinical Leadership in Mental Health Nursing. 2007. Available from:
2014;6:75–83. http://repository.digitalnz.org/system/uploads/record/attachment/195/
2. Doherty J. Improving Public Hospitals through Effective Clinical Leader- the_way_things_are_done_around_here__perceptions_of_clini-
ship, Lessons from South Africa. Johannesburg: 2014. Available from: cal_leadership_in_mental_health_nursing.pdf. Accessed May 24, 2017.
https://www.wits.ac.za/media/migration/files/cs-38933-fix/migrated- 23. Stanley D, Cuthbertson J, Latimer K. Perceptions of clinical leadership
pdf/pdfs-5/Clinical leadership report V4.pdf. Accessed May 24, 2017. in the St John Ambulance Service in WA. Response. 2013;39(1):31–37.
3. Wong CA, Cummings GG, Ducharme L. The relationship between 24. Stanley D, Blanchard D, Hohol A, Hutton M, McDonald A. Health
For personal use only.
nursing leadership and patient outcomes: a systematic review update. professionals’ perceptions of clinical leadership. A pilot study. Cogent
J Nurs Manag. 2013;21(5):709–724. Med. 2017;4(1)1321193.
4. National Committee for the Confidential Enquiry into Maternal Deaths. 25. British Medical Association. Doctors’ Perspectives on Clinical
Saving Mothers 2011-2013: Sixth Report on the Confidential Enquiry Leadership. London: 2012. Available from: https://www.bma.org.
into Maternal Deaths in South Africa. Pretoria: National Committee uk/connecting-doctors/search?q=Doctors%E2%80%99%20perspec-
for the Confidential Enquiry into Maternal Deaths; 2014. tives%20on%20clinical%20leadership. Accessed August 4, 2016.
5. Pattinson R, Rhoda N. Saving Babies 2012-2013: Ninth Report on 26. Jonas S, McCay L, Keogh B. The importance of clinical leadership. In:
Perinatal Care in South Africa for the PPIP Group. Pretoria: Tshepesa Swanwick T, McKimm J, editors. ABC of Clinical Leadership. 1st ed.
Press; 2014. Available from: http://www.ppip.co.za/wp-content/uploads/ Oxford: Blackwell Publishing Ltd; 2011:1–3. Available from: https://
Saving-Babies-2012-2013.pdf. Accessed May 23, 2017. scele.ui.ac.id/berkas_kolaborasi/konten/MKK_2014genap/ABC.pdf.
6. Pattinson R. Improving emergency obstetric care. Int J Gynecol Obstet. Accessed May 22, 2017.
2010;110(2):87–88. 27. Doherty J. Strengthening Clinical Leadership in Hospitals: A Review of
7. Van den Broek N [webpage on the Internet]. Life Saving Skills Manual: the International and South African Literature. Johannesburg: Municipal
Essential Obstetric and Newborn Care. 2nd ed. Cambridge University Service Project; 2013. Available from: https://www.wits.ac.za/media/
Press; 2007. Available from: https://www.amazon.co.uk/Life-Saving- migration/files/cs-38933-fix/migrated-pdf/pdfs-5/Strengthening clinical
Skills-Manual-Essential/dp/1107654742. Accessed May 24, 2017. leadership in hospitalsVers2.pdf. Accessed May 23, 2017.
8. Doherty JE, Couper ID, Campbell D, Walker J. Transforming rural 28. National Health Services Institute for Innovation and Improvement.
health systems through clinical academic leadership: lessons from Shared leadership underpinning of the MLCF. Enhancing Engagement
South Africa. Rural Remote Health. 2013;13(2):2618. in Medical Leadership. Coventry: 2009. Available from: http://www.
9. Mountford J, Webb C. When clinicians lead | McKinsey & Company. leadershipacademy.nhs.uk/wp-content/uploads/2012/10/776bc9c27b6
McKinsey Q. 2009;2:44–53. e8741d0ff42e593ba44cf.pdf. Accessed May 24, 2017.
10. Casey M, McNamara M, Fealy G, Geraghty R. Nurses’ and midwives’ 29. Lunenburg FC. Power and leadership: an influence process. Int J Manag
clinical leadership development needs: a mixed methods study. J Adv Bus Admin. 2012;15(1). Available from: https://pdfs.semanticscholar.
Nurs. 2011;67(7):1502–1513. org/7965/8afc91bc9b8a8966f3827e372e3656c7bfce.pdf. Accessed May
11. Davidson P, Elliot D, Daly J. Clinical leadership in contemporary 24, 2017.
clinical practice: implications for nursing in Australia. J Nurs Manag. 30. Al-Sawai A. Leadership of healthcare professionals: where do we stand?
2006;14(3):180–187. Oman Med J. 2013;28(4):285–287.
12. Patrick A, Laschinger HK, Wong C, Finegan J. Developing and testing 31. Giltinane L. Leadership styles and theories. Nurs Stand. 2013;27(41):
a new measure of staff nurse clinical leadership: the clinical leadership 35–39.
survey. J Nurs Manag. 2011;19(4):449–460. 32. Hagbaghery M, IMahvash S, Fazlolah A. The factors facilitating and
13. Curtis EA, de Vries J, Sheerin FK. Developing leadership in nursing: inhibiting effective clinical decision-making in nursing: a qualitative
exploring core factors. Br J Nurs. 2011;20(5):306–309. study. BMC Nurs. 2004;3(1):2.
14. McNamara MS, Fealy GM, Casey M, et al. Boundary matters: clinical 33. Patton C [webpage on the Internet]. Conflict in health care: a literature
leadership and the distinctive disciplinary contribution of nursing to review. Int J Healthc Admin. 2014;9(1). Available from: http://ispub.
multidisciplinary care. J Clin Nurs. 2011;20(23–24):3502–3512. com/IJHCA/9/1/20081. Accessed May 24, 2017.
15. Pickering C, Grignon J, Steven R, Guitart D, Byrne J. Publishing not 34. Fairholm MR. Different perspectives on the practice of leadership.
perishing: how research students transition from novice to knowledge- Public Adm Rev. 2015;64(5):577–590.
able using systematic quantitative literature reviews. Stud Higher Educ. 35. Slide C. The five intelligences of leadership. Leader Leader. 2007;
2015;40(10):1756–1769. 43:19–26.
86 submit your manuscript | www.dovepress.com Journal of Healthcare Leadership 2017:9
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Conceptualizations of clinical leadership
Journal of Healthcare Leadership downloaded from https://www.dovepress.com/ by 114.7.8.218 on 15-Apr-2021
For personal use only.
Journal of Healthcare Leadership Dovepress
Publish your work in this journal
The Journal of Healthcare Leadership is an international, peer-reviewed, open Interdisciplinary decision-making; Philosophical and ethical issues; Hazard
access journal focusing on leadership for the health profession. The journal is management; Research and opinion for health leadership; Leadership assess-
committed to the rapid publication of research focusing on but not limited to: ment. The manuscript management system is completely online and includes
Healthcare policy and law; Theoretical and practical aspects of healthcare deliv- a very quick and fair peer-review system. Visit http://www.dovepress.com/
ery; Interactions between healthcare and society and evidence-based practices; testimonials.php to read real quotes from published authors.
Submit your manuscript here: http://www.dovepress.com/journal-of-healthcare-leadership-journal
Journal of Healthcare Leadership 2017:9 submit your manuscript | www.dovepress.com
87
Dovepress
Powered by TCPDF (www.tcpdf.org)
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- NSHE - Hostile Work Environment ComplaintDocument21 pagesNSHE - Hostile Work Environment ComplaintJacob Solis67% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Enhanced Erpat ManualDocument167 pagesEnhanced Erpat ManualNeil Sabijon88% (42)
- Exam in Community Engagement Solidarity & CitizenshipDocument4 pagesExam in Community Engagement Solidarity & Citizenshiplovelyjanemartin100% (8)
- Organizational Diagnostic ModelsDocument36 pagesOrganizational Diagnostic ModelsSHRAVANI MEGHAVATHNo ratings yet
- 8 Coaching ModelsDocument4 pages8 Coaching ModelsGirish Jha100% (3)
- Introduction To ManagementDocument4 pagesIntroduction To ManagementRizal Chan100% (1)
- 13 Functions of ManagersDocument4 pages13 Functions of ManagersBalawin Dananau100% (1)
- Supply Chain MGMTDocument22 pagesSupply Chain MGMThimanshu111992No ratings yet
- Process Overview Business Relationship Management ItilDocument1 pageProcess Overview Business Relationship Management ItilrkamundimuNo ratings yet
- Disaster Preparedness: Hospital Decontamination and The Pediatric Patient-Guidelines For Hospitals and Emergency PlannersDocument9 pagesDisaster Preparedness: Hospital Decontamination and The Pediatric Patient-Guidelines For Hospitals and Emergency PlannersBayu PrabuNo ratings yet
- Leadership and Management Competencies For Hospital Managers: A Systematic Review and Best-Fit Framework SynthesisDocument10 pagesLeadership and Management Competencies For Hospital Managers: A Systematic Review and Best-Fit Framework SynthesisBayu PrabuNo ratings yet
- Review Article Teledentistry: A Boon Amidst COVID-19 Lockdown - A Narrative ReviewDocument6 pagesReview Article Teledentistry: A Boon Amidst COVID-19 Lockdown - A Narrative ReviewBayu PrabuNo ratings yet
- Soal Chapter 2 Bahasa InggrisDocument8 pagesSoal Chapter 2 Bahasa InggrisBayu PrabuNo ratings yet
- An Unmet Need in Healthcare Leadership: A Survey of Practicing Physicians' Perspectives On Healthcare Delivery Science EducationDocument8 pagesAn Unmet Need in Healthcare Leadership: A Survey of Practicing Physicians' Perspectives On Healthcare Delivery Science EducationBayu PrabuNo ratings yet
- JHL 255093 The Career Core of Successful Scientific Leaders in NursingDocument9 pagesJHL 255093 The Career Core of Successful Scientific Leaders in NursingBayu PrabuNo ratings yet
- JHL 120166 Leadership Requirements For Lean Versus Servant Leadership I 011817Document14 pagesJHL 120166 Leadership Requirements For Lean Versus Servant Leadership I 011817Bayu PrabuNo ratings yet
- The Relationship Between Leadership Style and Health Worker Motivation, Job Satisfaction and Teamwork in UgandaDocument12 pagesThe Relationship Between Leadership Style and Health Worker Motivation, Job Satisfaction and Teamwork in UgandaBayu PrabuNo ratings yet
- JHL 141664 Developing A Model For Effective Leadership in Healthcare A 082817Document10 pagesJHL 141664 Developing A Model For Effective Leadership in Healthcare A 082817Bayu PrabuNo ratings yet
- JHL 80011 Assment of The Management Factors Which Influence The Develo - 030215Document11 pagesJHL 80011 Assment of The Management Factors Which Influence The Develo - 030215Bayu PrabuNo ratings yet
- JHL 15620 Improving Heathcare Quality Through Culturally Competent Phys - 021411Document12 pagesJHL 15620 Improving Heathcare Quality Through Culturally Competent Phys - 021411Bayu PrabuNo ratings yet
- Research Article: Integration of 5G and Block-Chain Technologies in Smart Telemedicine Using IotDocument18 pagesResearch Article: Integration of 5G and Block-Chain Technologies in Smart Telemedicine Using IotBayu PrabuNo ratings yet
- JHL 139029 Corrigendum Ottawa Model of Implementation Leadership o Mil 050517Document1 pageJHL 139029 Corrigendum Ottawa Model of Implementation Leadership o Mil 050517Bayu PrabuNo ratings yet
- Research Article Telerehabilitation Using Fitness Application in Patients With Severe Cystic Fibrosis Awaiting Lung Transplant: A Pilot StudyDocument7 pagesResearch Article Telerehabilitation Using Fitness Application in Patients With Severe Cystic Fibrosis Awaiting Lung Transplant: A Pilot StudyBayu PrabuNo ratings yet
- Research Article: Design and Customization of Telemedicine SystemsDocument17 pagesResearch Article: Design and Customization of Telemedicine SystemsBayu PrabuNo ratings yet
- How To Shape Your Reputation As A LeaderDocument3 pagesHow To Shape Your Reputation As A LeaderNyoNo ratings yet
- BP A ShellDocument19 pagesBP A Shelldarshan_zamwarNo ratings yet
- Followership 1 (ST-002 FOLLOWERSHIP)Document51 pagesFollowership 1 (ST-002 FOLLOWERSHIP)DebbieNo ratings yet
- SPS Danielson FrameworkDocument15 pagesSPS Danielson FrameworkJulian A.100% (1)
- Ihrm NotesDocument3 pagesIhrm NotesNeha KashyapNo ratings yet
- Business Today September 10 2017Document127 pagesBusiness Today September 10 2017pramod kumarNo ratings yet
- NAyatel ReportDocument112 pagesNAyatel ReportMehwish Pervaiz100% (1)
- EthicsDocument23 pagesEthicsSouravAgarwalNo ratings yet
- Educ-10 Chapter 3 Group ActDocument6 pagesEduc-10 Chapter 3 Group ActAliah MosqueraNo ratings yet
- Leadership and Management Guiding Principles, Best.15 PDFDocument2 pagesLeadership and Management Guiding Principles, Best.15 PDFMarcus OsórioNo ratings yet
- Crusade Mission Pack: Beyond The Veil: Updates & ErrataDocument6 pagesCrusade Mission Pack: Beyond The Veil: Updates & ErrataSocioNo ratings yet
- Canadian Advertising in Action Keith TuckwellDocument1,560 pagesCanadian Advertising in Action Keith TuckwellStanzin YutungNo ratings yet
- Principal of Management (MGT 201) Spring - Section Course InstructorDocument16 pagesPrincipal of Management (MGT 201) Spring - Section Course InstructorSaieed AfridiNo ratings yet
- City of Richmond Employee Salaries-2022-10Document192 pagesCity of Richmond Employee Salaries-2022-10OpenOversightVA.orgNo ratings yet
- BUS 6070 FinalProjectDocument10 pagesBUS 6070 FinalProjectHafsat Saliu100% (2)
- Recruitment and Retention Strategy 2014 - 2017 PDFDocument33 pagesRecruitment and Retention Strategy 2014 - 2017 PDFMiha68No ratings yet
- PQM Consultants Compro 2019 - R4Document23 pagesPQM Consultants Compro 2019 - R4Emad HamdiNo ratings yet
- The Impact of Motivation On Job SatisfactionDocument120 pagesThe Impact of Motivation On Job Satisfactionnazch007100% (1)
- Module 5 Mice Lecture Notes 5Document8 pagesModule 5 Mice Lecture Notes 5SHIRLEY S. QuintoNo ratings yet
- Management - Nepali BBS 3rd YearDocument63 pagesManagement - Nepali BBS 3rd YearDhurba Bahadur BkNo ratings yet
- Topic 2 - Human Resource Management Strategy and AnalysisDocument25 pagesTopic 2 - Human Resource Management Strategy and AnalysisSHEIKH MUHAMMAD SAADNo ratings yet