You might also like
- Clinical Approach To Respiratory Distress in NewbornDocument29 pagesClinical Approach To Respiratory Distress in Newbornabhivnair100% (1)
- Nursing the NeonateFrom EverandNursing the NeonateMaggie MeeksNo ratings yet
- Allergic Rhinitis in Children: Diagnosis and TreatmentDocument39 pagesAllergic Rhinitis in Children: Diagnosis and Treatmentrinajacky100% (2)
- Nursing Care of Newborn AssessmentDocument15 pagesNursing Care of Newborn AssessmentMary RoseNo ratings yet
- Hackam 2022 - Bench To Bedside - New Insights Into The Pathogenesis of Necrotizing EnterocolitisDocument12 pagesHackam 2022 - Bench To Bedside - New Insights Into The Pathogenesis of Necrotizing EnterocolitisBee GuyNo ratings yet
- Neonatal SubgalealDocument6 pagesNeonatal SubgalealIrenLayNo ratings yet
- Allergic Rhinitis in Children: A Common but Treatable ConditionDocument7 pagesAllergic Rhinitis in Children: A Common but Treatable ConditionTina MorleyNo ratings yet
- 05 Polycythemia in The NewbornDocument11 pages05 Polycythemia in The NewbornMorales Eli PediatraNo ratings yet
- Mother and Child Protection Card: Paste Photo of Child HereDocument32 pagesMother and Child Protection Card: Paste Photo of Child HereMoham'medAlthafAs'lam100% (1)
- Neonatal Transition: Training of The Trainers Neonatal ResuscitationDocument36 pagesNeonatal Transition: Training of The Trainers Neonatal ResuscitationmitaNo ratings yet
- A Neonate With Acute Kidney Injury: Case PresentationDocument4 pagesA Neonate With Acute Kidney Injury: Case PresentationSahil DhamijaNo ratings yet
- Neonatal Resuscitation. Advances in Training and PracticeDocument10 pagesNeonatal Resuscitation. Advances in Training and PracticeFer45No ratings yet
- Kenya Immunization ScheduleDocument1 pageKenya Immunization ScheduleDani AnyikaNo ratings yet
- Neonatal JaundiceDocument63 pagesNeonatal JaundiceMade Oka HeryanaNo ratings yet
- 21321Document56 pages21321Daniel TabalanzaNo ratings yet
- Neonatal AssessmentDocument14 pagesNeonatal Assessmentkingpin@mailinator100% (1)
- Primary Health Care: Dr. Ariful Bari ChowdhuryDocument39 pagesPrimary Health Care: Dr. Ariful Bari ChowdhuryTanni ChowdhuryNo ratings yet
- Physical Growth and Development: Different Aspects and AssessmentDocument60 pagesPhysical Growth and Development: Different Aspects and AssessmentDipti RamiNo ratings yet
- Mechanical Ventilation of The Neonate Principles and StrategiesDocument6 pagesMechanical Ventilation of The Neonate Principles and StrategiesKelly HoffmanNo ratings yet
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDocument12 pagesMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RNo ratings yet
- Acute Malnutrition - Roxas City 100214Document70 pagesAcute Malnutrition - Roxas City 100214Geline Joy D. SamillanoNo ratings yet
- DOH Maternal Health ProgramDocument5 pagesDOH Maternal Health ProgramErwin Jake TagubaNo ratings yet
- 9, Procedure of PICCDocument9 pages9, Procedure of PICCputriseptinaNo ratings yet
- Pediatric Malignant Bone TumoursDocument28 pagesPediatric Malignant Bone TumourscorneliusNo ratings yet
- Management of Neonatal HypoglycemiaDocument14 pagesManagement of Neonatal Hypoglycemiaece142No ratings yet
- Care of A Client With: Neonatal Pneumonia: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu CityDocument22 pagesCare of A Client With: Neonatal Pneumonia: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu CityAsterlyn ConiendoNo ratings yet
- Newborn Respiratory Distress 11.28.2011Document41 pagesNewborn Respiratory Distress 11.28.2011Emily EresumaNo ratings yet
- Febrile convulsions: assessment, treatment and educationDocument12 pagesFebrile convulsions: assessment, treatment and educationPalash NagdeoteNo ratings yet
- Newborn ResuscitationDocument57 pagesNewborn ResuscitationmateenNo ratings yet
- Nurse PicuDocument5 pagesNurse PicuDitto RezkiawanNo ratings yet
- Division of Perinatology Department of Child Health Medical School University of Sumatera UtaraDocument37 pagesDivision of Perinatology Department of Child Health Medical School University of Sumatera UtaraJosephine IrenaNo ratings yet
- Respiratory Distress Management in NewbornDocument5 pagesRespiratory Distress Management in Newbornagirl_9807100% (1)
- Acute Liver Failure in Children and Adolescents 2012 Clinics and Research in Hepatology and GastroenterologyDocument6 pagesAcute Liver Failure in Children and Adolescents 2012 Clinics and Research in Hepatology and Gastroenterologyarshi_pimNo ratings yet
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNo ratings yet
- Skills For Care Presentation Web Version Standard 3Document16 pagesSkills For Care Presentation Web Version Standard 3pitr134No ratings yet
- Hemorrhagic Disease of Newborn PDFDocument2 pagesHemorrhagic Disease of Newborn PDFIndah Paradifa SariNo ratings yet
- Congenital SyphilisDocument6 pagesCongenital SyphilisFrozen Pandora MahayaNo ratings yet
- CPR - Cardiopulmonary ResuscitationDocument31 pagesCPR - Cardiopulmonary ResuscitationPanji HerlambangNo ratings yet
- Neonatal Emergencies FinalDocument90 pagesNeonatal Emergencies FinalDr Raseena VattamkandathilNo ratings yet
- Interatitial Lung DiseaseDocument2 pagesInteratitial Lung DiseaseIsabel CastilloNo ratings yet
- 5 Bleeding Disorders PPT EditedDocument87 pages5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNo ratings yet
- What Is The Glasgow Coma Scale?: BrainlineDocument4 pagesWhat Is The Glasgow Coma Scale?: BrainlineHershey ArenasNo ratings yet
- Anemia of PrematurityDocument14 pagesAnemia of PrematurityMariel HuamancayoNo ratings yet
- Golden Hours Management of High Risk Newborns - 2019Document10 pagesGolden Hours Management of High Risk Newborns - 2019Suryadi LimardiNo ratings yet
- Recommended Standards For Newborn ICU DesignDocument18 pagesRecommended Standards For Newborn ICU DesignYayang Andayani100% (1)
- Ten Steps to Successful BreastfeedingDocument42 pagesTen Steps to Successful BreastfeedingKwin IbaliNo ratings yet
- Neonatal SepsisDocument17 pagesNeonatal SepsisDhilla Feroh Kesuma TNo ratings yet
- HydronephrosisDocument2 pagesHydronephrosisGanis RyNo ratings yet
- Retinopathy of Prematurity (ROP) - 2019Document14 pagesRetinopathy of Prematurity (ROP) - 2019Suhail RafikNo ratings yet
- FLUID MANAGEMENT IN MALNUTRITIONDocument30 pagesFLUID MANAGEMENT IN MALNUTRITIONCHALIE MEQUNo ratings yet
- Fundal Height ScreeningDocument10 pagesFundal Height ScreeningDr_Soranus100% (1)
- Fix Care of NewbornDocument39 pagesFix Care of Newborngratzia fionaNo ratings yet
- Critical Care Update PDFDocument25 pagesCritical Care Update PDFHugo PozoNo ratings yet
- Perioperative Fluid Management in ChildrenDocument31 pagesPerioperative Fluid Management in ChildrenRashmi SahaNo ratings yet
- InTech-Neonatal Pneumonia PDFDocument14 pagesInTech-Neonatal Pneumonia PDFClaudia PalominoNo ratings yet
- MusQan National Quality Assurance Standards and Assessment Tools For DH and CHCDocument274 pagesMusQan National Quality Assurance Standards and Assessment Tools For DH and CHCRahul JalauniaNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Vit E, K, Minerals Def.Document39 pagesVit E, K, Minerals Def.Josselle Sempio CalientaNo ratings yet
- CHAPTER 63 and 64 Vitamin CDocument41 pagesCHAPTER 63 and 64 Vitamin CJosselle Sempio CalientaNo ratings yet
- Development and Evaluation of A New Igm/Igg Rapid Diagnostic Test For Sars-Cov-2Document8 pagesDevelopment and Evaluation of A New Igm/Igg Rapid Diagnostic Test For Sars-Cov-2Josselle Sempio CalientaNo ratings yet
- Nelson's Hour - 58-60Document51 pagesNelson's Hour - 58-60Josselle Sempio CalientaNo ratings yet
- Nutritional Requirements: Christine Mae R. Cando Pediatric Resident DjnrmhsDocument52 pagesNutritional Requirements: Christine Mae R. Cando Pediatric Resident DjnrmhsJosselle Sempio CalientaNo ratings yet
- Pphn. Nursing Grand Rounds. April 2. 2020 - FinalDocument154 pagesPphn. Nursing Grand Rounds. April 2. 2020 - FinalJosselle Sempio CalientaNo ratings yet
- Headss For AdolescentsDocument7 pagesHeadss For AdolescentsSamer FarhanNo ratings yet
- Eclia-20200823 180625Document19 pagesEclia-20200823 180625SANDHYASINI NAYAKNo ratings yet
- Meta Ana Article For ParticipantsDocument16 pagesMeta Ana Article For ParticipantsJosselle Sempio CalientaNo ratings yet
- 368 FullDocument8 pages368 FullWindy MentariiNo ratings yet
- Study of Electrolyte Disturbances in Dengue Infected PatientsDocument4 pagesStudy of Electrolyte Disturbances in Dengue Infected PatientsJosselle Sempio CalientaNo ratings yet
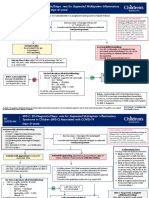
- MIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesMIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenJosselle Sempio CalientaNo ratings yet
- Pneumonia and Respiratory Tract Infections in ChildrenDocument37 pagesPneumonia and Respiratory Tract Infections in ChildrenjayasiinputNo ratings yet
- Hydrocephalus and Anomalies of the CNS: Embryology and PathologyDocument127 pagesHydrocephalus and Anomalies of the CNS: Embryology and PathologyJosselle Sempio CalientaNo ratings yet
- AAP 2017 Guidelines for Childhood HypertensionDocument81 pagesAAP 2017 Guidelines for Childhood HypertensionMira Mariana UlfahNo ratings yet
- Solcoseryl Improves Liquor Volume and Outcomes in IUGR BabiesDocument7 pagesSolcoseryl Improves Liquor Volume and Outcomes in IUGR BabiesJosselle Sempio CalientaNo ratings yet
- Adolescent HEADDSDocument3 pagesAdolescent HEADDSmoganrasaNo ratings yet
- Adolescent HEADDSDocument3 pagesAdolescent HEADDSmoganrasaNo ratings yet
- FSDFSDFSDFSDFSDDocument4 pagesFSDFSDFSDFSDFSDylessinNo ratings yet
- Issuance of Dangerous Drugs License (S2-License, Practitioner)Document4 pagesIssuance of Dangerous Drugs License (S2-License, Practitioner)Josselle Sempio CalientaNo ratings yet
- Mechanisms of Action of Zinc in Acute DiarrheaDocument6 pagesMechanisms of Action of Zinc in Acute DiarrheaJosselle Sempio Calienta100% (1)
- Taming The Beasts: Top Killers of Children: Pneumonia, A Global PerspectiveDocument24 pagesTaming The Beasts: Top Killers of Children: Pneumonia, A Global PerspectiveGelynM.TyNo ratings yet
- (Name) (Civil Status) (Complete Home Address) : AffidavitDocument1 page(Name) (Civil Status) (Complete Home Address) : AffidavitJosselle Sempio Calienta100% (1)
- Nervous CaputDocument5 pagesNervous CaputVellyana GustikaNo ratings yet
- CPG On Dengue in Children 2017Document108 pagesCPG On Dengue in Children 2017Hannah LeiNo ratings yet
- PPSDocument7 pagesPPSJosselle Sempio CalientaNo ratings yet
- Fluid Management in Neonates and InfantsDocument51 pagesFluid Management in Neonates and InfantsSulabh Shrestha100% (1)
- DioxelDocument1 pageDioxelJosselle Sempio CalientaNo ratings yet
- Fluid Management in Neonates and InfantsDocument14 pagesFluid Management in Neonates and InfantsJosselle Sempio CalientaNo ratings yet
- Paediatrics Respiratory Distress in The NewbornDocument15 pagesPaediatrics Respiratory Distress in The NewbornEddy Lopez GuerreroNo ratings yet
- Neonatal Pneumonia UpToDateDocument34 pagesNeonatal Pneumonia UpToDateKhayelee PalosNo ratings yet
- Nursing Care of A Family With A High Risk NewbornDocument68 pagesNursing Care of A Family With A High Risk NewbornJennie CortezNo ratings yet
- 4 Meconium Aspiration SyndromeDocument30 pages4 Meconium Aspiration SyndromeRana Vandana100% (2)
- Respiratory Distress Syndrome (Hyaline Membrane Disease)Document98 pagesRespiratory Distress Syndrome (Hyaline Membrane Disease)Miraf MesfinNo ratings yet
- Respiratory Distress SyndromeDocument69 pagesRespiratory Distress SyndromeAbraham ChiuNo ratings yet
- Meconium Aspiration Syndrome, Management ofDocument9 pagesMeconium Aspiration Syndrome, Management ofGinaJaraNo ratings yet
- Pathophysiology of Meconium AspirationDocument4 pagesPathophysiology of Meconium AspirationMarcus Luke L. Dauz100% (1)
- Meconium Aspiration Syndrome: Causes, Symptoms and TreatmentDocument13 pagesMeconium Aspiration Syndrome: Causes, Symptoms and TreatmentSANANo ratings yet
- Meconium Aspiration Syndrome: Causes, Symptoms and TreatmentDocument38 pagesMeconium Aspiration Syndrome: Causes, Symptoms and TreatmentGrace Antonette Pati100% (1)
- The Factors Affecting Persistent Pneumothorax and Mortality in Neonatal PneumothoraxDocument5 pagesThe Factors Affecting Persistent Pneumothorax and Mortality in Neonatal PneumothoraxRahardi MokhtarNo ratings yet
- Perinatal Asphyxia in Term and Late Preterm Infants - UpToDateDocument31 pagesPerinatal Asphyxia in Term and Late Preterm Infants - UpToDateRocio GNo ratings yet
- Causes, Severity and Outcome of Neonatal Thrombocytopenia in Hi-Tech Medical College and Hospital, BhubaneswarDocument4 pagesCauses, Severity and Outcome of Neonatal Thrombocytopenia in Hi-Tech Medical College and Hospital, BhubaneswarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Respiratory Distress in The Newborn: Pediatrics in Review October 2014Document16 pagesRespiratory Distress in The Newborn: Pediatrics in Review October 2014turigauNo ratings yet
- All Pediatrics 2Document200 pagesAll Pediatrics 2niemand daNo ratings yet
- Meconium Aspiration SyndromeDocument7 pagesMeconium Aspiration SyndromeAi Niech Inoel100% (1)
- Neonatal Respiratory DisordersDocument68 pagesNeonatal Respiratory Disorderslordoftheweb100% (25)
- Respiratory Distress in NewbornDocument7 pagesRespiratory Distress in NewbornChimot Ona MilanelloNo ratings yet
- High Risk New BornDocument36 pagesHigh Risk New BornIze C VijiNo ratings yet
- Common Diseases of NewbornDocument162 pagesCommon Diseases of NewbornMichelle ThereseNo ratings yet
- High Risk NewbornDocument20 pagesHigh Risk Newborndmrdy50% (2)
- Meconium Passage in UteroDocument12 pagesMeconium Passage in UteroJennifer IbarraNo ratings yet
- OB HESI Study GuideDocument34 pagesOB HESI Study GuideLeah Hunter97% (35)
- NCM 109 MidtermDocument12 pagesNCM 109 MidtermApril Maecy F. DignomoNo ratings yet
- Meconium Aspiration Syndrome & Transient Tachypnea of The NewbornDocument20 pagesMeconium Aspiration Syndrome & Transient Tachypnea of The NewbornArianne AlaveNo ratings yet
- NUR 145 Lecture 2 Term 2Document184 pagesNUR 145 Lecture 2 Term 2Maria Jonalyn Bautista RodelasNo ratings yet
- Causes and Outcomes of Respiratory Distress in NeonatesDocument8 pagesCauses and Outcomes of Respiratory Distress in NeonatesMohammad AlmuhaiminNo ratings yet
- Endrenal Reyzelin M.-Concept Map & NCPDocument5 pagesEndrenal Reyzelin M.-Concept Map & NCPReyzelinNo ratings yet
- Illness in The NewbornDocument34 pagesIllness in The NewbornVivian Jean TapayaNo ratings yet
- Meconium Aspiration Syndrome: DR Bob KlajoDocument17 pagesMeconium Aspiration Syndrome: DR Bob KlajoBob John100% (1)