You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Arab Board Orthopedic Exam June 2013Document35 pagesArab Board Orthopedic Exam June 2013doos150% (2)
- Strengthening Primary Health Care Through Community Health WorkersDocument26 pagesStrengthening Primary Health Care Through Community Health WorkersRawNo ratings yet
- (Accompagnateurs OR Activista OR "Agente Comunitario deDocument30 pages(Accompagnateurs OR Activista OR "Agente Comunitario deRawNo ratings yet
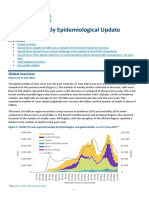
- Weekly Epi Update 46Document19 pagesWeekly Epi Update 46RawNo ratings yet
- Advert - 6th Eachsc Bujumbura - Burundi - 29-31 March 2017Document3 pagesAdvert - 6th Eachsc Bujumbura - Burundi - 29-31 March 2017RawNo ratings yet
- HCC AASLD Practice Guidance 2023Document104 pagesHCC AASLD Practice Guidance 202333newman33No ratings yet
- Bio8 Report Assignment5Document56 pagesBio8 Report Assignment5AliNo ratings yet
- Communicable DiseasesDocument161 pagesCommunicable DiseasesNader Smadi95% (20)
- Historical OVERVIEW On Blood BankingDocument4 pagesHistorical OVERVIEW On Blood BankingSogan, MaureenNo ratings yet
- Prevalence of Hepatitis B Virus Infection and Related Risk Factors in A Rural Community of MexicoDocument5 pagesPrevalence of Hepatitis B Virus Infection and Related Risk Factors in A Rural Community of MexicoEmmanuel LawerNo ratings yet
- Rapid Assessment of Viral Hepatitis Testing and Quality AssuranceDocument18 pagesRapid Assessment of Viral Hepatitis Testing and Quality AssuranceCHELSIE KAITLYN DE GUZMANNo ratings yet
- EASL HepBDocument42 pagesEASL HepBmutiara dewiNo ratings yet
- Directory of Service (DOS) - Effective From 1st April 2012Document74 pagesDirectory of Service (DOS) - Effective From 1st April 2012kgnmatinNo ratings yet
- Hepatitis B: Journal ReviewDocument41 pagesHepatitis B: Journal Reviewagita kartika sariNo ratings yet
- Hepatitis B in PregnancyDocument12 pagesHepatitis B in PregnancyTasya Felicia MacellinNo ratings yet
- Bioline Rapid. Urinalysis TestDocument34 pagesBioline Rapid. Urinalysis Testvan luomNo ratings yet
- Recombinant VaccinesDocument22 pagesRecombinant VaccinesjugesmangangNo ratings yet
- JaundiceDocument17 pagesJaundiceDarwithaNo ratings yet
- MCQ's For TrainingDocument52 pagesMCQ's For TrainingYalvant YadavNo ratings yet
- General Principles and Overview of Management of Rheumatoid Arthritis in Adults - UpToDateDocument32 pagesGeneral Principles and Overview of Management of Rheumatoid Arthritis in Adults - UpToDateImad RifayNo ratings yet
- Hepatitis B (HBV) : 2-Months RegimenDocument20 pagesHepatitis B (HBV) : 2-Months Regimenulovemusicsodoi7799No ratings yet
- HepBPerinatal ProtectWhenPregnant BWDocument2 pagesHepBPerinatal ProtectWhenPregnant BWKhalidatunnur Andrianie NasihinNo ratings yet
- Immunology Practice Questions With AnswersDocument21 pagesImmunology Practice Questions With AnswersBigBoosting100% (2)
- Nss 505 Medical Surgical Nursing Critical Care I Teacher - Co .KeDocument171 pagesNss 505 Medical Surgical Nursing Critical Care I Teacher - Co .Kebirhanu Ayenew AnleyNo ratings yet
- Oral RevalidaDocument3 pagesOral RevalidaJaye DangoNo ratings yet
- 07 - JMV 2010Document11 pages07 - JMV 2010sunilpkumar18No ratings yet
- Preventive ObstetricsDocument57 pagesPreventive ObstetricsGunaNo ratings yet
- Hepatobiliary ExamDocument10 pagesHepatobiliary ExamAllison Eunice Servando100% (1)
- Lilypad Learning Center Staff HandbookDocument41 pagesLilypad Learning Center Staff HandbookPrabha GuptaNo ratings yet
- Pediatric Hepatitis B Treatment: Haruki Komatsu, Ayano Inui, Tomoo FujisawaDocument13 pagesPediatric Hepatitis B Treatment: Haruki Komatsu, Ayano Inui, Tomoo FujisawaDarmawan HariyantoNo ratings yet
- Hepatitis B PDFDocument8 pagesHepatitis B PDFponekNo ratings yet
- Love Letter PDFDocument31 pagesLove Letter PDFAlan Kintanar IIINo ratings yet
- Hepatitis: Charles Manoj Chauhan Vedprakash Thakur AlokDocument29 pagesHepatitis: Charles Manoj Chauhan Vedprakash Thakur AlokCk LamaNo ratings yet
- Development and Characterization of Herbal Nanopaticle of Genistein For The Treatment of Hepatic Cellular Carcinoma (4) - 3Document18 pagesDevelopment and Characterization of Herbal Nanopaticle of Genistein For The Treatment of Hepatic Cellular Carcinoma (4) - 3VOOGLS PUBLICATIONNo ratings yet