You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Infective EndocarditisDocument18 pagesInfective EndocarditisLee Foo WengNo ratings yet
- Harris Hip ScoreDocument2 pagesHarris Hip ScoreRicky Aris Fandika50% (2)
- Infectious DiseasesDocument62 pagesInfectious DiseasesakufahabaNo ratings yet
- Food Borne Diseases Associated With Foods of Animal OriginDocument60 pagesFood Borne Diseases Associated With Foods of Animal OriginWan SyarifuddinNo ratings yet
- Specialconsiderationobturatorhernia 110210102125 Phpapp02Document17 pagesSpecialconsiderationobturatorhernia 110210102125 Phpapp02Ricky Aris FandikaNo ratings yet
- Diverticulardiseasecolon 130106062944 Phpapp02Document79 pagesDiverticulardiseasecolon 130106062944 Phpapp02Ricky Aris FandikaNo ratings yet
- Radiationproctitis 090421073253 Phpapp02Document18 pagesRadiationproctitis 090421073253 Phpapp02Ricky Aris FandikaNo ratings yet
- 2015 Primary Breast Sarcoma A Retrospective Study Over 35 Years From A Single InstitutionDocument8 pages2015 Primary Breast Sarcoma A Retrospective Study Over 35 Years From A Single InstitutionRicky Aris FandikaNo ratings yet
- Primary Breast Sarcoma: A Rare Pathology in Women From The National Cancer Institute (Incan) of MexicoDocument3 pagesPrimary Breast Sarcoma: A Rare Pathology in Women From The National Cancer Institute (Incan) of MexicoRicky Aris FandikaNo ratings yet
- Neoadjuvant Chemotherapy For Primary Sarcoma of The Breast: A Case ReportDocument6 pagesNeoadjuvant Chemotherapy For Primary Sarcoma of The Breast: A Case ReportRicky Aris FandikaNo ratings yet
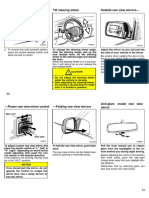
- Tilt Steering Wheel Outside Rear View MirrorsDocument3 pagesTilt Steering Wheel Outside Rear View MirrorsRicky Aris FandikaNo ratings yet
- Primary Breast Sarcoma: Clinicopathologic Series From The Mayo Clinic and Review of The LiteratureDocument5 pagesPrimary Breast Sarcoma: Clinicopathologic Series From The Mayo Clinic and Review of The LiteratureRicky Aris FandikaNo ratings yet
- A Scary Onset of A Rare and Aggressive Type of Primary Breast Sarcoma: A Case ReportDocument6 pagesA Scary Onset of A Rare and Aggressive Type of Primary Breast Sarcoma: A Case ReportRicky Aris FandikaNo ratings yet
- 2008 Evaluation and Management of Persistent Problems After Surgery For Hirschsprung Disease in A ChildDocument7 pages2008 Evaluation and Management of Persistent Problems After Surgery For Hirschsprung Disease in A ChildRicky Aris FandikaNo ratings yet
- Download textbook Basic Medical Microbiology Patrick R Murray ebook all chapter pdfDocument53 pagesDownload textbook Basic Medical Microbiology Patrick R Murray ebook all chapter pdflaura.fenton551100% (16)
- Case Files® EnterococcusDocument4 pagesCase Files® EnterococcusAHMAD ADE SAPUTRANo ratings yet
- Treatment Mapping UTI Ranges and Reporting1Document7 pagesTreatment Mapping UTI Ranges and Reporting1Shehraz TariqNo ratings yet
- Bacte Compilation PDFDocument83 pagesBacte Compilation PDFAnne MorenoNo ratings yet
- Lower Susquehanna Subbasin Small Watershed Study: Yellow Breeches Creek, A Bacteriological Assessment, February - November 2006Document20 pagesLower Susquehanna Subbasin Small Watershed Study: Yellow Breeches Creek, A Bacteriological Assessment, February - November 2006srbc100% (2)
- Presented by MR S. Jugroo (PMSM) : National Dialysis Coordinator Ministry of Health and WellnessDocument56 pagesPresented by MR S. Jugroo (PMSM) : National Dialysis Coordinator Ministry of Health and WellnessKhedu VeemlaNo ratings yet
- Biological and Physicochemical Indicators of Water Quality in Libreville and Its SurroundingsDocument7 pagesBiological and Physicochemical Indicators of Water Quality in Libreville and Its SurroundingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 22 Streptococcus, Enterococcus and PneumococcusDocument73 pagesChapter 22 Streptococcus, Enterococcus and PneumococcusPriyanshiNo ratings yet
- Streptococcus and EnterococcusDocument91 pagesStreptococcus and EnterococcusAllyah Ross DuqueNo ratings yet
- Infectious Diseases of The Female Genital TractDocument1,111 pagesInfectious Diseases of The Female Genital TractJohn Ntokos100% (2)
- Daptomycin 5Document2 pagesDaptomycin 5SachithNo ratings yet
- Antibiotic Resistance in Wastewater BacteriaDocument14 pagesAntibiotic Resistance in Wastewater BacteriaraowaleedahmadNo ratings yet
- Central Line Infection PathwayDocument36 pagesCentral Line Infection PathwaycignalNo ratings yet
- Uji Deteksi Biofilm Dari Isolat Klinik Kateter Urin Bakteri Entercoccus Dibandingkan Dengan Tube MethodDocument27 pagesUji Deteksi Biofilm Dari Isolat Klinik Kateter Urin Bakteri Entercoccus Dibandingkan Dengan Tube MethodIyannyanNo ratings yet
- Evaluation of Antimicrobial Activity of ZITRITIDEDocument16 pagesEvaluation of Antimicrobial Activity of ZITRITIDEednisoNo ratings yet
- RAPID AST FROM BLOOD CULUTURE-Methodology - EUCAST - RAST - v1 - 20181126 PDFDocument3 pagesRAPID AST FROM BLOOD CULUTURE-Methodology - EUCAST - RAST - v1 - 20181126 PDFKhoa Vi Sinh BVCRNo ratings yet
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Document12 pagesIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNo ratings yet
- E FaecalisDocument5 pagesE FaecalisShyambhavi SrivastavaNo ratings yet
- 2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2Document13 pages2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2giseladlrNo ratings yet
- Escherichia Coli, and Enteric: Enteric Indicator Organisms in FoodsDocument7 pagesEscherichia Coli, and Enteric: Enteric Indicator Organisms in Foodssiddharth2907No ratings yet
- 2023 Assessment of Vibrio SPP Abundance As A Water Quality Indicator-Insights From Mali Ston Bay in The Adriatic SeaDocument10 pages2023 Assessment of Vibrio SPP Abundance As A Water Quality Indicator-Insights From Mali Ston Bay in The Adriatic SeaindahbioNo ratings yet
- Bile Aesuclin Azide Agar: ApplicationDocument3 pagesBile Aesuclin Azide Agar: ApplicationJimmy Rodríguez JuárezNo ratings yet
- Antimicrobial ResistanceDocument46 pagesAntimicrobial ResistanceEmil CotenescuNo ratings yet
- TDS SlanetzDocument4 pagesTDS SlanetzDiana DiasNo ratings yet
- The Efficacy of Piper Betle Linn Against Methicillin Resistant Staphylococcus Aureus and Vancomycin-Resistant EnterococcusDocument20 pagesThe Efficacy of Piper Betle Linn Against Methicillin Resistant Staphylococcus Aureus and Vancomycin-Resistant EnterococcusClaire GonoNo ratings yet
- Vantocil Ib - Hopital ApplicationDocument3 pagesVantocil Ib - Hopital ApplicationMinh LêNo ratings yet