You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Sirkulus Wilisi: David C. R 112019011Document32 pagesSirkulus Wilisi: David C. R 112019011David ChristianNo ratings yet
- Keratitis Acanthamoeba Jamur Dan Bakteri Perbandingan Faktor RisikoDocument12 pagesKeratitis Acanthamoeba Jamur Dan Bakteri Perbandingan Faktor RisikoDavid ChristianNo ratings yet
- Radio FMDocument2 pagesRadio FMDavid ChristianNo ratings yet
- 464 13 746 1 10 20170929Document12 pages464 13 746 1 10 20170929Widy SilambaNo ratings yet
- Denver PrintDocument1 pageDenver PrintDavid ChristianNo ratings yet
- Ekg Pada SkaDocument25 pagesEkg Pada SkaJonathan Karel GunawanNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
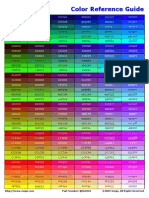
- Color Reference GuideDocument3 pagesColor Reference GuideMiha4No ratings yet
- 12lect Intro Graphic Design 2017bDocument31 pages12lect Intro Graphic Design 2017btayimdavid17No ratings yet
- DA1 RoboticsDocument3 pagesDA1 RoboticsViswanadh VankamamidiNo ratings yet
- The Color Thresholder App: Excerpted From The BlogDocument7 pagesThe Color Thresholder App: Excerpted From The BlogM Xubair Yousaf XaiNo ratings yet
- Comparison of Goldmann Applanation Tonometer, Tono-PenDocument19 pagesComparison of Goldmann Applanation Tonometer, Tono-PenLidiasilambaNo ratings yet
- Serial Kasus Tatalaksana Retinopathy of Prematurity ROP - Andreas Lukita HalimDocument15 pagesSerial Kasus Tatalaksana Retinopathy of Prematurity ROP - Andreas Lukita HalimEko NoviantiNo ratings yet
- What Is Visual Acuity and Why Do NDT Technicians Need ItDocument1 pageWhat Is Visual Acuity and Why Do NDT Technicians Need ItnavitaNo ratings yet
- What Is An Epiretinal Membrane?Document6 pagesWhat Is An Epiretinal Membrane?Chip MorrisNo ratings yet
- PL V2 Series Product Introduction V1.8-20230505Document32 pagesPL V2 Series Product Introduction V1.8-20230505eventlighting.auNo ratings yet
- The Physiology of VisionDocument24 pagesThe Physiology of VisionSana MohsinNo ratings yet
- Color Communication & MatchingDocument46 pagesColor Communication & Matchingtrường phạmNo ratings yet
- Nemosys-Xr™: Range of Optronic Solutions Designed For Extra Long Distance SurveillanceDocument2 pagesNemosys-Xr™: Range of Optronic Solutions Designed For Extra Long Distance SurveillanceMohd Syafiq bin MortadaNo ratings yet
- Apple 12Document116 pagesApple 12Choo Wei shengNo ratings yet
- 25 - Corneal Edema After PhacoemulsificationDocument10 pages25 - Corneal Edema After PhacoemulsificationOphthalmology Resident UNSRAT manado 2017No ratings yet
- Digital Perfect PhotographyDocument2 pagesDigital Perfect PhotographyAlex CostaNo ratings yet
- Kuliah Glaukoma Unila Dr. RaniDocument57 pagesKuliah Glaukoma Unila Dr. RaniCaesarioNo ratings yet
- A Beginner's Guide To Screen Printing, by A Complete BeginnerDocument21 pagesA Beginner's Guide To Screen Printing, by A Complete BeginnerMd Aslam ShahNo ratings yet
- Cable ColorDocument4 pagesCable ColorNghia Huynh Ngoc0% (1)
- Simulating A Genuine Silver-Gelatin Image: Step 1Document11 pagesSimulating A Genuine Silver-Gelatin Image: Step 1mbrethenNo ratings yet
- Computer Graphics Panning, Clipping, SegmentationDocument17 pagesComputer Graphics Panning, Clipping, SegmentationMaryam javeriaNo ratings yet
- Nikon Z50 Settings and PhotosDocument27 pagesNikon Z50 Settings and Photosgp.mishraNo ratings yet
- FCB Ex1000Document2 pagesFCB Ex1000Vany BraunNo ratings yet
- DIP IMP QB (E-Next - In)Document6 pagesDIP IMP QB (E-Next - In)Aishwarya SonawaneNo ratings yet
- Askeb. Komunitas Kematian Maternal Dan NeonatalDocument36 pagesAskeb. Komunitas Kematian Maternal Dan NeonatalAnita A.e.sNo ratings yet
- How To Calibrate Your Equipment Using Color BarsDocument6 pagesHow To Calibrate Your Equipment Using Color BarsAnirban GhoseNo ratings yet
- Image CompressionDocument41 pagesImage Compressionchetanajitesh76No ratings yet
- Fact Sheets (Biology)Document2 pagesFact Sheets (Biology)Samantha GoNo ratings yet
- Lunar Brand Guide - CutDocument10 pagesLunar Brand Guide - CutHunter RosenblumeNo ratings yet
- LU6 Ang, GGT Ophtha251 CataractAssignmentDocument2 pagesLU6 Ang, GGT Ophtha251 CataractAssignmentPJ PJNo ratings yet
- BCSC Reading Schedule 2020-2021Document13 pagesBCSC Reading Schedule 2020-2021StefanieNo ratings yet