0% found this document useful (0 votes)
59 views3 pagesVisitor Health Declaration Form
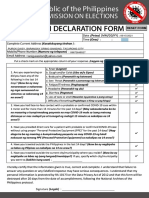
The visitor health declaration form collects personal information such as name, age, temperature, residence, and contact number. It asks a series of yes or no questions regarding COVID-19 symptoms, close contact with COVID-19 cases, travel history, and contact with others exhibiting symptoms. By signing, the visitor authorizes the organization to collect and process this health data to control the spread of COVID-19, and acknowledges their requirement to provide truthful information according to relevant acts.
Uploaded by
Gena Fe L. JagusCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
59 views3 pagesVisitor Health Declaration Form
The visitor health declaration form collects personal information such as name, age, temperature, residence, and contact number. It asks a series of yes or no questions regarding COVID-19 symptoms, close contact with COVID-19 cases, travel history, and contact with others exhibiting symptoms. By signing, the visitor authorizes the organization to collect and process this health data to control the spread of COVID-19, and acknowledges their requirement to provide truthful information according to relevant acts.
Uploaded by
Gena Fe L. JagusCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd