You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Nursing Care Plan For Ineffective Breastfeeding NCPDocument4 pagesNursing Care Plan For Ineffective Breastfeeding NCPderic76% (46)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NCP BreastfeedingDocument3 pagesNCP BreastfeedingLeo FrivaldoNo ratings yet
- 18 - The Nuts and Bolts of BF Anatomy and PhysiologyDocument6 pages18 - The Nuts and Bolts of BF Anatomy and PhysiologysasNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Document27 pagesParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- Parathyroid Surgery For Inherited Syndromes - Uptodate 2022Document25 pagesParathyroid Surgery For Inherited Syndromes - Uptodate 2022juanrangoneNo ratings yet
- Intraoperative Parathyroid Hormone Assays - Uptodate 2022Document18 pagesIntraoperative Parathyroid Hormone Assays - Uptodate 2022juanrangoneNo ratings yet
- 1 A History Fo Melanoma - From Hunter To Morton Sober2019Document19 pages1 A History Fo Melanoma - From Hunter To Morton Sober2019juanrangoneNo ratings yet
- 9 Biopsy of The Sentinel Lymph NodeDocument32 pages9 Biopsy of The Sentinel Lymph NodejuanrangoneNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- 23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomaDocument19 pages23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomajuanrangoneNo ratings yet
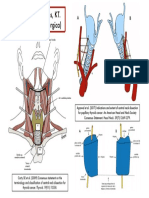
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDocument1 pageNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
- Anatomy of The Superficial Fascia System of The Breast: A Comprehensive Theory of Breast Fascial AnatomyDocument10 pagesAnatomy of The Superficial Fascia System of The Breast: A Comprehensive Theory of Breast Fascial AnatomyLuiggi FayadNo ratings yet
- AnsaCervicalis Chhetri1997Document7 pagesAnsaCervicalis Chhetri1997ita mustainahNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Vandeventer 2016Document10 pagesVandeventer 2016juanrangoneNo ratings yet
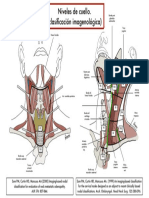
- Clasif Imagenológica Niveles de CuelloDocument1 pageClasif Imagenológica Niveles de CuellojuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document5 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- Breast ExaminationDocument3 pagesBreast ExaminationShum Wing Hei JoanneNo ratings yet
- Leaflets Ward ClassDocument5 pagesLeaflets Ward ClassJustine CagatanNo ratings yet
- Jurnal Pijat Oksitosin Upload 1Document5 pagesJurnal Pijat Oksitosin Upload 1Silfa RianyNo ratings yet
- 2020 Breastfeeding WatermarkDocument83 pages2020 Breastfeeding WatermarkJasmin T. RegaspiNo ratings yet
- Breast Complications: Presented by Sridevi Devaraj Asst - Lecturer Kcon BangaloreDocument15 pagesBreast Complications: Presented by Sridevi Devaraj Asst - Lecturer Kcon BangaloreSridevi DevarajNo ratings yet
- MastitisDocument25 pagesMastitisCHRISTIAN SIDAYANo ratings yet
- CX LinksDocument9 pagesCX LinksJosephe RaykáNo ratings yet
- Perbedaan Efektifitas Pemberian Buah Kurma Dan Daun Katuk Terhadap Kelancaran Asi Pada Ibu Menyusui Umur 0-40 Hari Di Kota KediriDocument7 pagesPerbedaan Efektifitas Pemberian Buah Kurma Dan Daun Katuk Terhadap Kelancaran Asi Pada Ibu Menyusui Umur 0-40 Hari Di Kota KediriDavid CahyaNo ratings yet
- X130Y AN IssueDocument30 pagesX130Y AN IssueCleano FaçanhaNo ratings yet
- Risk For Aspiration Related To Insufficient Parental Knowledge Regarding Breastfeeding TechniquesDocument2 pagesRisk For Aspiration Related To Insufficient Parental Knowledge Regarding Breastfeeding TechniquesNicolai MabituinNo ratings yet
- Breast Examination: DefinitionDocument3 pagesBreast Examination: Definitionsagi muNo ratings yet
- Lactational MastitisDocument2 pagesLactational MastitisMarijosse NavarroNo ratings yet
- (MIOMIO) ALL Types of Position (Breastfeeding)Document12 pages(MIOMIO) ALL Types of Position (Breastfeeding)Juliet Marie MiomioNo ratings yet
- Breastfeeding - Anatomy and PhysiologyDocument22 pagesBreastfeeding - Anatomy and PhysiologyGaylinel BongyadNo ratings yet
- Lactation ConsultantDocument7 pagesLactation Consultantapi-663756427No ratings yet
- Breast CareDocument5 pagesBreast CareBhawna Pandhu100% (2)
- Management of Breast EngorgementDocument2 pagesManagement of Breast EngorgementKathleen ColinioNo ratings yet
- PDF Biaya MaternityDocument2 pagesPDF Biaya MaternityKurnia Yuliyanti RahayuNo ratings yet
- Kacang Hijau TDHP Produksi ASIDocument10 pagesKacang Hijau TDHP Produksi ASIRohmi HandayaniNo ratings yet
- What Is The Tanner Staging System?: Stage OneDocument2 pagesWhat Is The Tanner Staging System?: Stage OneSriLestariFajerinNo ratings yet
- Bfhi-Session-5-How Breastfeeding WorksDocument16 pagesBfhi-Session-5-How Breastfeeding Worksreema arshadNo ratings yet
- Duct EctasiaDocument6 pagesDuct EctasiaChristopher MhagamaNo ratings yet
- Mercy Health Boardman Lactation Powerpoint PresentationDocument12 pagesMercy Health Boardman Lactation Powerpoint Presentationapi-607727110No ratings yet
- Brassiere Fitting GuideDocument1 pageBrassiere Fitting GuideLinette CabreraNo ratings yet
- Mentor® Product Guide: Global BrandDocument32 pagesMentor® Product Guide: Global BrandIgor GrisendiNo ratings yet
- 5 Laws of Natural Breast LiftDocument8 pages5 Laws of Natural Breast LiftwhisperssNo ratings yet
- Breast Pumps Flyer EN 1819-Single-Pages-A4Document6 pagesBreast Pumps Flyer EN 1819-Single-Pages-A4Rigoberto Leigue OrdoñezNo ratings yet