You might also like
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
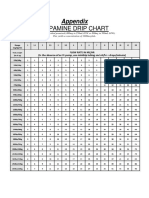
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
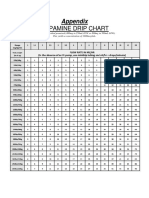
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- Zhou2019 Article InsulinDegludecANovelUltra-LonDocument18 pagesZhou2019 Article InsulinDegludecANovelUltra-LonmehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
- Anak - Kasus 7 - Kelompok 7Document48 pagesAnak - Kasus 7 - Kelompok 7mehakNo ratings yet
- The Correlation of Structural and Binding Affinity of Insulin Analog To The Onset of Action For Diabetic TherapyDocument9 pagesThe Correlation of Structural and Binding Affinity of Insulin Analog To The Onset of Action For Diabetic TherapymehakNo ratings yet
- This Content Downloaded From 202.43.95.25 On Tue, 05 Oct 2021 01:35:52 UTCDocument8 pagesThis Content Downloaded From 202.43.95.25 On Tue, 05 Oct 2021 01:35:52 UTCmehakNo ratings yet
- Kementerian Pendidikan, Kebudayaan Riset Dan Teknologi: Direktorat Jenderal Pendidikan TinggiDocument11 pagesKementerian Pendidikan, Kebudayaan Riset Dan Teknologi: Direktorat Jenderal Pendidikan TinggimehakNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DigoxinDocument6 pagesDigoxinSEIYADU IBRAHIM KNo ratings yet
- Extrinsic Regulation of The HeartDocument9 pagesExtrinsic Regulation of The Heartkawaiijanai gfNo ratings yet
- 2014 Aha/Acc Guidelines For The Management of Patients With Non-St-Elevation Acute Coronary SyndromeDocument10 pages2014 Aha/Acc Guidelines For The Management of Patients With Non-St-Elevation Acute Coronary Syndromefarah0001No ratings yet
- Hipertensi UrgensiDocument26 pagesHipertensi UrgensidiegoNo ratings yet
- Materi DR Rita Zahara NewDocument31 pagesMateri DR Rita Zahara NewIrfanNo ratings yet
- Why Worry About: High Blood Pressure?Document8 pagesWhy Worry About: High Blood Pressure?mattvestrandNo ratings yet
- FDC - IrrationalDocument30 pagesFDC - Irrationaldivya lohithNo ratings yet
- Management of Hypertensive Crisis: British and Irish Hypertension Society Position DocumentDocument17 pagesManagement of Hypertensive Crisis: British and Irish Hypertension Society Position DocumentPaula SantosNo ratings yet
- Drug Therapy For Angina Pectoris - Pak WilarDocument3 pagesDrug Therapy For Angina Pectoris - Pak WilarVikneswaran VîçkýNo ratings yet
- Free Drug Bank GUIDE 1 PDFDocument76 pagesFree Drug Bank GUIDE 1 PDFRaouf Ra'fat Soliman100% (11)
- Pharmacology CardiovascularDocument86 pagesPharmacology Cardiovascularamasoud96 amasoud96No ratings yet
- Vasodilators and The Treatment of Angina PectorisDocument24 pagesVasodilators and The Treatment of Angina PectorisKriselda May TorioNo ratings yet
- Nicardipine DripDocument8 pagesNicardipine DripRichard Ines ValinoNo ratings yet
- Effective, Modern Directions in The Prevention and Treatment of Pulmonary Hypertension in Patients With Bronchial Asthma (Literature Review)Document13 pagesEffective, Modern Directions in The Prevention and Treatment of Pulmonary Hypertension in Patients With Bronchial Asthma (Literature Review)Central Asian StudiesNo ratings yet
- Risk Factors Pathophysiology and Management of HypertensionDocument13 pagesRisk Factors Pathophysiology and Management of HypertensionDominggas RusunwullyNo ratings yet
- Antianginal Drugs.. Prof. Dr. Adeeb Al-ZubaidyDocument19 pagesAntianginal Drugs.. Prof. Dr. Adeeb Al-ZubaidySara AbbasNo ratings yet
- All Past Rounds Cardio MCQs AlexandriaDocument37 pagesAll Past Rounds Cardio MCQs AlexandriaMahmoud Abouelsoud100% (1)
- Lec 22 ANTIHYPERTENSIVE - 2Document22 pagesLec 22 ANTIHYPERTENSIVE - 2Abdul MananNo ratings yet
- NCLEX Select All That Apply Practice Exam 4Document8 pagesNCLEX Select All That Apply Practice Exam 4Heather ClemonsNo ratings yet
- Massage Therapy and MedicationsOxfordDocument232 pagesMassage Therapy and MedicationsOxfordboutique.chersNo ratings yet
- Pharm MnemonicsDocument33 pagesPharm MnemonicsThomson George75% (4)
- List of Common Drugs and Their AntidotesDocument2 pagesList of Common Drugs and Their AntidotesMourian AmanNo ratings yet
- Cardiology Lectures 1 4 DR - Deduyo PDFDocument31 pagesCardiology Lectures 1 4 DR - Deduyo PDFMiguel Cuevas DolotNo ratings yet
- Pharmacology Semi FinalsDocument269 pagesPharmacology Semi FinalsTrishaNo ratings yet
- Topnotch Pharma Supertable JAN 2016Document166 pagesTopnotch Pharma Supertable JAN 2016Dar AD50% (2)
- 6.3 Neuro Case PresDocument25 pages6.3 Neuro Case PresJane StarkNo ratings yet
- MORAES-SILVA Et Al 2017Document20 pagesMORAES-SILVA Et Al 2017Luiza MartinsNo ratings yet
- 2017 Medical Pharmacology Practice Exam 4Document6 pages2017 Medical Pharmacology Practice Exam 4Franklin garryNo ratings yet
- Publication Upload120426593487001335425842HIPERTENSI SmallDocument68 pagesPublication Upload120426593487001335425842HIPERTENSI SmallZidni Arifa LuthfiNo ratings yet
- اسئله باطني مدققه 740823Document42 pagesاسئله باطني مدققه 740823Ashraf AlbhlaNo ratings yet