You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CT Scanner Asteion Super 4 PDFDocument16 pagesCT Scanner Asteion Super 4 PDFYusef ManasrahNo ratings yet
- ASTM D 558-96 Standard Method For Misture-Density Relations of Soil-Cement MixturesDocument5 pagesASTM D 558-96 Standard Method For Misture-Density Relations of Soil-Cement MixturesPablo Antonio Valcárcel Vargas50% (2)
- TM-1861 AVEVA Administration (1.4) System Administration Rev 1.0Document106 pagesTM-1861 AVEVA Administration (1.4) System Administration Rev 1.0praveen jangir100% (2)
- Јohn Lakos - Large-Scale C++ Volume I - Process and Architecture (2020, Pearson)Document1,023 pagesЈohn Lakos - Large-Scale C++ Volume I - Process and Architecture (2020, Pearson)asdasd asdasdNo ratings yet
- HVAC Listing - Addendum #1Document3 pagesHVAC Listing - Addendum #1Jhonny Velasquez PerezNo ratings yet
- C+source Code On +scienific CalculatorDocument22 pagesC+source Code On +scienific CalculatorBittu76% (29)
- Documents - Pub - Boardworks LTD 2004 1 of 27 A4 Sequences ks3 MathematicsDocument69 pagesDocuments - Pub - Boardworks LTD 2004 1 of 27 A4 Sequences ks3 MathematicsYan EnNo ratings yet
- Module2-Signals and SystemsDocument21 pagesModule2-Signals and SystemsAkul PaiNo ratings yet
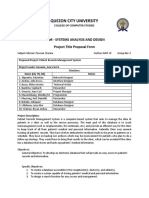
- Group 1 Revised Proposal. Patient Records Management SystemDocument2 pagesGroup 1 Revised Proposal. Patient Records Management SystemAlioding M. MacarimbangNo ratings yet
- International Journal of Accounting & Information ManagementDocument23 pagesInternational Journal of Accounting & Information ManagementAboneh TeshomeNo ratings yet
- Manual de Usuario Ecografo DC40 PDFDocument291 pagesManual de Usuario Ecografo DC40 PDFFederico Rodriguez MonsalveNo ratings yet
- Pay Order Application-Bangla-englishDocument1 pagePay Order Application-Bangla-englishTasnim RaihanNo ratings yet
- Jumbo C Saver CatalogueDocument19 pagesJumbo C Saver CatalogueMuhammad Iqbal ANo ratings yet
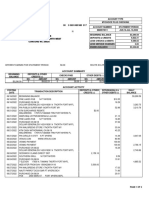
- Fetch Statementand NoticesDocument4 pagesFetch Statementand NoticesElizabethNo ratings yet
- Icon Line Trimmer - ICPLT26 Operator ManualDocument10 pagesIcon Line Trimmer - ICPLT26 Operator ManualAnirudh Merugu67% (3)
- Voice ProcedureDocument246 pagesVoice ProcedureManaf Kwame Osei Asare100% (1)
- OTC Family of Battery Testers: Sabre HPDocument4 pagesOTC Family of Battery Testers: Sabre HPenticoNo ratings yet
- MT131 Tutorial - 2 Sets Functions Sequences and Summation - 2023-2024Document63 pagesMT131 Tutorial - 2 Sets Functions Sequences and Summation - 2023-2024johnnader1254No ratings yet
- Innovation ManagementDocument39 pagesInnovation Managementmoraiskp321No ratings yet
- Ficha Tecnica Rotametro 7510 PDFDocument2 pagesFicha Tecnica Rotametro 7510 PDFJohn Armely Arias GuerreroNo ratings yet
- VU Provider For CS619 2021-2022Document10 pagesVU Provider For CS619 2021-2022zeeshan dogarNo ratings yet
- BSP Pipe ThreadDocument1 pageBSP Pipe ThreadgvmindiaNo ratings yet
- Lecture 5. Industry 4.0 Technologies and Enterprise ArchitectureDocument13 pagesLecture 5. Industry 4.0 Technologies and Enterprise ArchitectureBobo SevenNo ratings yet
- Hafiz CVDocument6 pagesHafiz CVkashi4ashiNo ratings yet
- Christmas Tree Safety TipsDocument1 pageChristmas Tree Safety Tipskailashch.msihraNo ratings yet
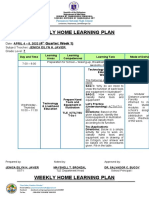
- Weekly Home Learning Plan: (4 Quarter: Week 1)Document8 pagesWeekly Home Learning Plan: (4 Quarter: Week 1)JenicaEilynNo ratings yet
- Cropyield Prediction Using Flask AND Machine LearningDocument11 pagesCropyield Prediction Using Flask AND Machine LearningVenkata Nikhil Chakravarthy KorrapatiNo ratings yet
- Full Catalog 2023 - Email VerDocument80 pagesFull Catalog 2023 - Email VeradamNo ratings yet
- Types of Circuit BreakersDocument23 pagesTypes of Circuit Breakerspmankad60% (5)
- Mn00224e-ALPlus2 - ALCPlus2 - ALCPlus2eDocument388 pagesMn00224e-ALPlus2 - ALCPlus2 - ALCPlus2eAlberto Rodrigues de SouzaNo ratings yet