
You might also like
- Autism Pathways To Recovery Book by DR AmyDocument247 pagesAutism Pathways To Recovery Book by DR Amypurecuban99100% (3)
- 6 Week Program From Mass Made SimpleDocument40 pages6 Week Program From Mass Made SimpleNicolas VeraNo ratings yet
- Cancer Cures Cancer Treatments That Work - Top 10 Natural Cancer TreatmentsDocument8 pagesCancer Cures Cancer Treatments That Work - Top 10 Natural Cancer TreatmentsDr. Dennis Clark100% (1)
- Cancer Risks From WiFi and Mobile Phones Review of Evidence (2011)Document7 pagesCancer Risks From WiFi and Mobile Phones Review of Evidence (2011)EMFsafetyNo ratings yet
- INTERNS NOTES - OtorhinolaryngologyDocument15 pagesINTERNS NOTES - OtorhinolaryngologyKarl Jimenez SeparaNo ratings yet
- Tumor Suppressor Gene & Proto-OncogeneDocument61 pagesTumor Suppressor Gene & Proto-OncogeneKartthik ShanmugamNo ratings yet
- How to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthFrom EverandHow to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthNo ratings yet
- Coping CancerDocument28 pagesCoping CancerCharlene TomasNo ratings yet
- Gelatin, Stress, Longevity Ray PeatDocument13 pagesGelatin, Stress, Longevity Ray Peatwxcvbnnbvcxw100% (1)
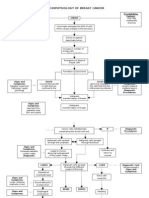
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Basic Principles of Radiation OncologyDocument34 pagesBasic Principles of Radiation OncologyEstiani Ningsih100% (1)
- Holistic and Non Medical TreatmentDocument17 pagesHolistic and Non Medical TreatmentMaina PeterNo ratings yet
- Case Study TabhsoDocument7 pagesCase Study TabhsoGina Barredo Bustamante100% (1)
- The Extra Oral and Intra Oral Examination: FeatureDocument3 pagesThe Extra Oral and Intra Oral Examination: Featuremuhammad nauvalNo ratings yet
- Encyclopedia of Controlled Drug Delivery (2 Vols) - E. Mathiowitz (Wiley, 1999) WWDocument903 pagesEncyclopedia of Controlled Drug Delivery (2 Vols) - E. Mathiowitz (Wiley, 1999) WWCiontu Valentin100% (4)
- Poorer Survival Outcomes For Male Breast Cancer Compared With Female Breast Cancer May Be Attributable To In-Stage MigrationDocument9 pagesPoorer Survival Outcomes For Male Breast Cancer Compared With Female Breast Cancer May Be Attributable To In-Stage MigrationabcdshNo ratings yet
- Hopee 33Document11 pagesHopee 33Gabrelle OgayonNo ratings yet
- CPT Cancer 6Document15 pagesCPT Cancer 6Guadalupe PérezNo ratings yet
- Nhs 12283Document8 pagesNhs 12283maithakeloayNo ratings yet
- Depression and Quality of Life Among Patients With Uterus CarcinomaDocument22 pagesDepression and Quality of Life Among Patients With Uterus CarcinomaFATIMENo ratings yet
- Name of Student Name of Instructor Course ID DateDocument18 pagesName of Student Name of Instructor Course ID DateNeelam shahzadiNo ratings yet
- Yeo Et AlDocument10 pagesYeo Et AlAna MoraisNo ratings yet
- Beckjord CompasDocument19 pagesBeckjord CompasAna MoraisNo ratings yet
- Unequal Quality in Cancer Pain ManagementDocument9 pagesUnequal Quality in Cancer Pain Managementapi-244230664No ratings yet
- Relationship Between Working Conditions and Mental Health of Migrants and Refugees/asylum Seekers vs. Natives in Europe: A Systematic ReviewDocument12 pagesRelationship Between Working Conditions and Mental Health of Migrants and Refugees/asylum Seekers vs. Natives in Europe: A Systematic ReviewmarconimatteoNo ratings yet
- Final Cancer Rehab Position PaperDocument15 pagesFinal Cancer Rehab Position PaperPralhad TalavanekarNo ratings yet
- Koko's Project 2 Submitted WorkDocument50 pagesKoko's Project 2 Submitted WorkNlemorusa PaschalineNo ratings yet
- Background of The Study: Kale, and Caroll, 2016)Document17 pagesBackground of The Study: Kale, and Caroll, 2016)Renz Eric Garcia UlandayNo ratings yet
- BerteroDocument10 pagesBerteroAna MoraisNo ratings yet
- Well-Being and Posttraumatic Growth in Unrelated Donor MarrowDocument7 pagesWell-Being and Posttraumatic Growth in Unrelated Donor MarrowLuizaNo ratings yet
- Kirkman Et Al. - Fertility and Motherhood After Breast Cancer... (2014) PDFDocument12 pagesKirkman Et Al. - Fertility and Motherhood After Breast Cancer... (2014) PDFCSNo ratings yet
- Cervical Cancer Prevention in Transgender Men: A Review: Version of Record Doi: 10.1111/1471-0528.16503Document13 pagesCervical Cancer Prevention in Transgender Men: A Review: Version of Record Doi: 10.1111/1471-0528.16503tavo823No ratings yet
- The Importance of Gender in Health ProblemsDocument6 pagesThe Importance of Gender in Health Problemsmohdisram26No ratings yet
- Prevalence and Risk Factors of Urinary Incontinence Among Estonian Postmenopausal WomenDocument7 pagesPrevalence and Risk Factors of Urinary Incontinence Among Estonian Postmenopausal WomenherryNo ratings yet
- Chapter 1 EditedDocument8 pagesChapter 1 Editedroneldayo62No ratings yet
- Arndt Et Al 2008Document8 pagesArndt Et Al 2008chatsashNo ratings yet
- Breast Cancer SurvivorsDocument30 pagesBreast Cancer Survivorsvinodksahu100% (1)
- Nurs 916scholarship Paper 3Document13 pagesNurs 916scholarship Paper 3api-214213767No ratings yet
- Cheung2013 Article AssociationOfHandgripStrengthWDocument13 pagesCheung2013 Article AssociationOfHandgripStrengthWAahna GuptaNo ratings yet
- [European Journal of Cancer Care 2010-dec 20 vol. 20 iss. 1] A.-G. LE CORROLLER-SORIANO_ A.-D. BOUHNIK_ M. PREAU_ L. MALAVOLT - Does cancer survivors' health-related quality of life depend on cancer type_ Findings from a large - libgen.liDocument9 pages[European Journal of Cancer Care 2010-dec 20 vol. 20 iss. 1] A.-G. LE CORROLLER-SORIANO_ A.-D. BOUHNIK_ M. PREAU_ L. MALAVOLT - Does cancer survivors' health-related quality of life depend on cancer type_ Findings from a large - libgen.liRounak JhawarNo ratings yet
- The Use of Healing Touch in Integrative Oncology: at A GlanceDocument8 pagesThe Use of Healing Touch in Integrative Oncology: at A GlancedikaNo ratings yet
- Hope, Burden or Risk FPDocument24 pagesHope, Burden or Risk FPDolores GalloNo ratings yet
- Dissertation Ovarian CancerDocument12 pagesDissertation Ovarian CancerWriteMyPaperForCheapCanada100% (1)
- Tradução 3Document12 pagesTradução 3Ana AlineNo ratings yet
- Zulfah Purwina - Publikasi Jurnal Internasional SciTePress (Proses)Document14 pagesZulfah Purwina - Publikasi Jurnal Internasional SciTePress (Proses)Zulfah PurwinaNo ratings yet
- Applied Nursing Research: Mi-Kyoung Cho, PHD, Apn, Gisoo Shin, PHD, RNDocument7 pagesApplied Nursing Research: Mi-Kyoung Cho, PHD, Apn, Gisoo Shin, PHD, RNJoecoNo ratings yet
- 17 Iajps17102017 PDFDocument3 pages17 Iajps17102017 PDFBaru Chandrasekhar RaoNo ratings yet
- The Effect of Depression On The Quality 0f Life of Patient With Cervical Cancer at Dr. Moewardi Hospital in SurakartaDocument8 pagesThe Effect of Depression On The Quality 0f Life of Patient With Cervical Cancer at Dr. Moewardi Hospital in SurakartaEndahNo ratings yet
- 29 110 3 PBDocument9 pages29 110 3 PBWidia WidanaNo ratings yet
- British Journal of CancerDocument8 pagesBritish Journal of CancerYesui EnkhbatNo ratings yet
- Filipou - 2016Document4 pagesFilipou - 2016TurboNo ratings yet
- Sample RORLDocument25 pagesSample RORLLj BerganioNo ratings yet
- AnlloDocument9 pagesAnlloAna MoraisNo ratings yet
- (+) Author AffiliationsDocument9 pages(+) Author AffiliationsMuhammadShahzadNo ratings yet
- InTech-Comparison of Genome Aberrations Between Early Onset and Late Onset Breast CancerDocument15 pagesInTech-Comparison of Genome Aberrations Between Early Onset and Late Onset Breast CancerMuhammad MaulanaNo ratings yet
- Cancers: Symptom Clusters in Survivorship and Their Impact On Ability To Work Among Cancer SurvivorsDocument11 pagesCancers: Symptom Clusters in Survivorship and Their Impact On Ability To Work Among Cancer SurvivorsSteve GannabanNo ratings yet
- Gender and Bladder CancerDocument11 pagesGender and Bladder CancernimaelhajjiNo ratings yet
- Effectiveness of Patient Navigator Interventions On Uptake of ColorectalDocument15 pagesEffectiveness of Patient Navigator Interventions On Uptake of ColorectalmaleticjNo ratings yet
- Womens Health Research Paper TopicsDocument5 pagesWomens Health Research Paper Topicsaflbrozzi100% (1)
- Gorantla Synthesis PaperDocument25 pagesGorantla Synthesis Paperapi-464986748No ratings yet
- Approach To CancerDocument7 pagesApproach To CancerArthur SmithNo ratings yet
- Epidemiology of Gastric Cancer and Helicobacter Pylori: Jonathan Volk and Julie ParsonnetDocument34 pagesEpidemiology of Gastric Cancer and Helicobacter Pylori: Jonathan Volk and Julie ParsonnetSa 'ng WijayaNo ratings yet
- Grounded Theory Sample PDFDocument12 pagesGrounded Theory Sample PDFKevin GardoseNo ratings yet
- Berg and Hayashi 2013 PDFDocument10 pagesBerg and Hayashi 2013 PDFRAMONA GABRIELA LEBADANo ratings yet
- Being in Suspense Awaiting Ca Mammae SurgeryDocument11 pagesBeing in Suspense Awaiting Ca Mammae SurgeryLEIDY TATIANA PADILLA GARCIANo ratings yet
- Quantitative Measures of Self-Reported Data On Abortion Morbidity: A Case Study in Madhya Pradesh, IndiaDocument10 pagesQuantitative Measures of Self-Reported Data On Abortion Morbidity: A Case Study in Madhya Pradesh, IndiaHeather HennessyNo ratings yet
- Summary of Sexual Health in Women Affected by Gynecologic or Breast CancerDocument6 pagesSummary of Sexual Health in Women Affected by Gynecologic or Breast CancerconnieberiNo ratings yet
- 10 KotepuiDocument5 pages10 KotepuiAlfeus GradyNo ratings yet
- Genetics and Molecular Biology of Cancer A Seminar PresentedDocument20 pagesGenetics and Molecular Biology of Cancer A Seminar PresentedMarshal GrahamNo ratings yet
- Basic and Clinical Endocrinology Up-To-DateDocument360 pagesBasic and Clinical Endocrinology Up-To-DateIrina Isac0% (1)
- Lifestyle and Dietary Factors in The Prevention of Lethal Prostate CancerDocument10 pagesLifestyle and Dietary Factors in The Prevention of Lethal Prostate CancerDale MckinneyNo ratings yet
- Motives For Sharing Illness Experiences On Twitter Conversations of Parents With Children Diagnosed With CancerDocument17 pagesMotives For Sharing Illness Experiences On Twitter Conversations of Parents With Children Diagnosed With CancerNicolas VeraNo ratings yet
- DocumentDocument17 pagesDocumentNicolas VeraNo ratings yet
- Illness and The Politics of Social Suffering: Towards A Critical Research Agenda in Health and Science StudiesDocument25 pagesIllness and The Politics of Social Suffering: Towards A Critical Research Agenda in Health and Science StudiesNicolas VeraNo ratings yet
- Volume 25, Issue 2 - Spring 2015 ISSN: 1181-912X (Print), 2368-8076 (Online)Document9 pagesVolume 25, Issue 2 - Spring 2015 ISSN: 1181-912X (Print), 2368-8076 (Online)Nicolas VeraNo ratings yet
- Feminist Perspectives On Peacebuilding ADocument9 pagesFeminist Perspectives On Peacebuilding ANicolas VeraNo ratings yet
- Leucemia Mieloide AgudaDocument22 pagesLeucemia Mieloide AgudaGustavo AngelesNo ratings yet
- Lymphoma: Diagnosis and TreatmentDocument8 pagesLymphoma: Diagnosis and TreatmentDindaNo ratings yet
- Breast CancerDocument18 pagesBreast CancerJohn AlcantaraNo ratings yet
- Package - Insert - 08814 - I - en - 30429 - CA 15-3 PDFDocument7 pagesPackage - Insert - 08814 - I - en - 30429 - CA 15-3 PDFadybaila4680No ratings yet
- Proposal - Pediatric Cancer AwarenessDocument4 pagesProposal - Pediatric Cancer Awarenessapi-272067917No ratings yet
- Phycocyanin A Potential Drug For Cancer TreatmentDocument14 pagesPhycocyanin A Potential Drug For Cancer TreatmentSrivatsava RajagopalanNo ratings yet
- September 15, Maple Ridge-Pitt Meadows NewsDocument33 pagesSeptember 15, Maple Ridge-Pitt Meadows NewsmapleridgenewsNo ratings yet
- How Earthquakes Happen: Contoh / Example of Explanation Text About EarthquakeDocument5 pagesHow Earthquakes Happen: Contoh / Example of Explanation Text About EarthquakeFitiyaNo ratings yet
- International Agency For Research On Cancer Monograms On The Evaluation of Carcinogenic Risks To HumansDocument454 pagesInternational Agency For Research On Cancer Monograms On The Evaluation of Carcinogenic Risks To HumansDaily FreemanNo ratings yet
- 2014 IIB Sant Pau Cientific ReportDocument284 pages2014 IIB Sant Pau Cientific ReportJepiNo ratings yet
- Myths of U.S. HealthcareDocument3 pagesMyths of U.S. HealthcarecherylsealatlargeNo ratings yet
- Breast Cancer Diagnosed During PregnancyDocument3 pagesBreast Cancer Diagnosed During PregnancyJonny CardenasNo ratings yet
- Il 6Document5 pagesIl 6Suresh KumawatNo ratings yet
- SARMS Powders Prices - David FromDocument1 pageSARMS Powders Prices - David FromOld World OrderNo ratings yet
- Robert Ryan Cancer ProtocolDocument104 pagesRobert Ryan Cancer ProtocolChris Ryan100% (1)
- Tre 295Document4 pagesTre 295Ahmed Ben BellaNo ratings yet
- GliomasDocument35 pagesGliomasRabbya Nasir 5No ratings yet
- Imrt, Igrt, SBRT Advances in The Treatment Planning and Delivery of RadiotherapyDocument1 pageImrt, Igrt, SBRT Advances in The Treatment Planning and Delivery of RadiotherapyPrasanth PNo ratings yet
- DANC280 Group Assignment 7Document4 pagesDANC280 Group Assignment 7Jacov SmithNo ratings yet
- Spss Sig 0.05Document14 pagesSpss Sig 0.05xetijoNo ratings yet





































![[European Journal of Cancer Care 2010-dec 20 vol. 20 iss. 1] A.-G. LE CORROLLER-SORIANO_ A.-D. BOUHNIK_ M. PREAU_ L. MALAVOLT - Does cancer survivors' health-related quality of life depend on cancer type_ Findings from a large - libgen.li](https://imgv2-2-f.scribdassets.com/img/document/659002428/149x198/64bd621ffc/1710527262?v=1)























































