2014 FLORIDA NOT FOR PROFIT CORPORATION ANNUAL REPORT FILED
DOCUMENT# N14292 May 12, 2014
Entity Name: 4108 AERIE IMMOKALEE, FRATERNAL ORDER OF EAGLES, Secretary of State
INC. CC5667744685
Current Principal Place of Business:
403 W NEW MARKET RD
IMMOKALEE, FL 34142
Current Mailing Address:
P.O.BOX 5063
IMMOKALEE, FL 34143
FEI Number: 59-2528160 Certificate of Status Desired: No
Name and Address of Current Registered Agent:
SANDERS, JULIUS H
1817 PAUL ST.
SUITE 2
FORT MYERS, FL 33901 US
The above named entity submits this statement for the purpose of changing its registered office or registered agent, or both, in the State of Florida.
SIGNATURE:
Electronic Signature of Registered Agent Date
Officer/Director Detail :
Title P Title S
Name COURTRIGHT, MARVIN Name SANDERS, JULIUS
Address 261 MATECUMBE LN Address 403 W NEW MARKET RD
City-State-Zip: NAPLES FL 34114 City-State-Zip: IMMOKALEE FL 34142
Title D Title T
Name THOMAS, CARL Name COOK, RALPH
Address P.O. BOX 202 Address 13433 LAMIRADA CR.
City-State-Zip: FELDA FL 33930-0202 City-State-Zip: WELLINGTON FL 33414
Title D
Name LIGHTNER, DAVID
Address PO BOX 5189
City-State-Zip: IMMOKALEE FL 34143
I hereby certify that the information indicated on this report or supplemental report is true and accurate and that my electronic signature shall have the same legal effect as if made under
oath; that I am an officer or director of the corporation or the receiver or trustee empowered to execute this report as required by Chapter 617, Florida Statutes; and that my name appears
above, or on an attachment with all other like empowered.
SIGNATURE: JULIUS SANDERS AGENT 05/12/2014
Electronic Signature of Signing Officer/Director Detail Date
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Med ListDocument1 pageMed ListGlendaNo ratings yet
- Med ListDocument1 pageMed ListGlendaNo ratings yet
- Med ListDocument1 pageMed ListGlendaNo ratings yet
- This Is A Work Order Confirmation SheetDocument1 pageThis Is A Work Order Confirmation SheetGlendaNo ratings yet
- Customer Agreement H2323-54557Document13 pagesCustomer Agreement H2323-54557GlendaNo ratings yet
- Christiano Alexander: Official Summary of VisitDocument2 pagesChristiano Alexander: Official Summary of VisitGlendaNo ratings yet
- Permanent General Assurance CorporationDocument7 pagesPermanent General Assurance CorporationGlendaNo ratings yet
- Tow BustersDocument3 pagesTow BustersGlendaNo ratings yet
- UnknownDocument1 pageUnknownGlendaNo ratings yet
- eyJpdiI6ImlURytlY2w5N3h0VXB3RVowM0pTeWc9PSIsInZhbHVlIjoiVXVQTnErUlFKUjFKOEVZZEFRN21KQT09IiwibWFjIjoiYmE1MTdmZmYyNzQ4OTgwZWZlOWIwY2ExNTBhMmRiMDliMTA3YzIwOTZlZTZjMzNiMTQ3N2ViZmVhM2E3MGUzNSJ9Document2 pageseyJpdiI6ImlURytlY2w5N3h0VXB3RVowM0pTeWc9PSIsInZhbHVlIjoiVXVQTnErUlFKUjFKOEVZZEFRN21KQT09IiwibWFjIjoiYmE1MTdmZmYyNzQ4OTgwZWZlOWIwY2ExNTBhMmRiMDliMTA3YzIwOTZlZTZjMzNiMTQ3N2ViZmVhM2E3MGUzNSJ9GlendaNo ratings yet
- Owner #1 Owner #1 Photo Id: Schedule of Ownership FormDocument5 pagesOwner #1 Owner #1 Photo Id: Schedule of Ownership FormGlendaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ieee 1010Document106 pagesIeee 1010Jose Antonio EstofaneroNo ratings yet
- Position PaperDocument4 pagesPosition PaperJoyce GarqueNo ratings yet
- Bank AlFalahDocument89 pagesBank AlFalahIrfan safdarNo ratings yet
- State Versus Path FunctionsDocument10 pagesState Versus Path FunctionsRohan RanaNo ratings yet
- Case Study Tata SteelDocument3 pagesCase Study Tata SteelAnkurNo ratings yet
- Second Floor Plan Roof Deck Plan: A B C A B CDocument1 pageSecond Floor Plan Roof Deck Plan: A B C A B CReden Mejico PedernalNo ratings yet
- Nevada Vs CasugaDocument8 pagesNevada Vs CasugaRimvan Le SufeorNo ratings yet
- UNIT-4 (HRM Updated)Document42 pagesUNIT-4 (HRM Updated)GAURAV SHARMANo ratings yet
- Bird Beaks and BillsDocument16 pagesBird Beaks and BillsWhatdNo ratings yet
- Your Vodafone Bill: Amount DueDocument2 pagesYour Vodafone Bill: Amount DueRahul PrakashNo ratings yet
- Uniform CPA Examination Questions May 1980 To November 1981Document260 pagesUniform CPA Examination Questions May 1980 To November 1981Adrienne GonzalezNo ratings yet
- Sonic The Hedgehog (2018) Issue #32 - Read SonicDocument2 pagesSonic The Hedgehog (2018) Issue #32 - Read SonicDamir WhiteNo ratings yet
- Dwnload Full Criminological Theory A Brief Introduction 4th Edition Miller Test Bank PDFDocument36 pagesDwnload Full Criminological Theory A Brief Introduction 4th Edition Miller Test Bank PDFkimbernonakaspro100% (15)
- Week 11 Contemporary World (Module 10)Document7 pagesWeek 11 Contemporary World (Module 10)camillaNo ratings yet
- Ark BibhaDocument9 pagesArk BibhaKrishna Consciousness0% (1)
- Preamble of The Indian ConstitutionDocument4 pagesPreamble of The Indian ConstitutionSupriyaNo ratings yet
- INGRAM - Grievance DetailsDocument2 pagesINGRAM - Grievance DetailsMohan KrishnaNo ratings yet
- SRPbillApril2023 - NgonDocument1 pageSRPbillApril2023 - NgonHACKMAN DARIUSNo ratings yet
- Dans, Jr. vs. PeopleDocument24 pagesDans, Jr. vs. Peopleanon_614984256No ratings yet
- Beaumont v. PrietoDocument22 pagesBeaumont v. PrietoJNMGNo ratings yet
- Financial Management757 8NpfYQinoODocument3 pagesFinancial Management757 8NpfYQinoOHarshhaa ZanjageNo ratings yet
- Labatagos Vs Sandiganbayan, 183 SCRA 415Document4 pagesLabatagos Vs Sandiganbayan, 183 SCRA 415AddAllNo ratings yet
- Legal Writing - Reply RejoinderDocument3 pagesLegal Writing - Reply RejoinderdNo ratings yet
- Milaad Un NabiDocument17 pagesMilaad Un Nabisheraz1212No ratings yet
- Emergency Capacity Building Project: Safety, Security & Civil / Military RelationsDocument36 pagesEmergency Capacity Building Project: Safety, Security & Civil / Military Relationseliasox123No ratings yet
- Liam Law Vs Olympic SawmillDocument2 pagesLiam Law Vs Olympic SawmillMikhail TignoNo ratings yet
- General LunaDocument4 pagesGeneral LunaLeezlleeh Jenice Obeso MonderoNo ratings yet
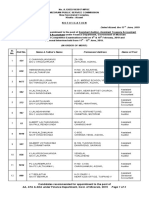
- Final Result of Aa Ada Ata Under Finance Department 2019Document3 pagesFinal Result of Aa Ada Ata Under Finance Department 2019Ab KhawlhringNo ratings yet
- United States v. Murphy, C.A.A.F. (2015)Document26 pagesUnited States v. Murphy, C.A.A.F. (2015)Scribd Government DocsNo ratings yet
- Siti Aisyah V PPDocument28 pagesSiti Aisyah V PPSyamimi SuhaimiNo ratings yet