You might also like
- The Lumbar MicrodiscectomyDocument5 pagesThe Lumbar Microdiscectomyokta fianNo ratings yet
- DIPJ Denervation Arenas-PratDocument3 pagesDIPJ Denervation Arenas-PratanindyaNo ratings yet
- Volar Henry Approach To The ForearmDocument4 pagesVolar Henry Approach To The ForearmJake sanchezNo ratings yet
- LWBK836 Ch98 p1021-1030Document10 pagesLWBK836 Ch98 p1021-1030metasoniko81No ratings yet
- Surgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDDocument9 pagesSurgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDGustavoBecerraNo ratings yet
- Rosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanDocument10 pagesRosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanMarcela RibeiroNo ratings yet
- DUR - Fracture of The Shaft Radius and UlnaDocument55 pagesDUR - Fracture of The Shaft Radius and UlnaM. Abdurrahman Al-HaraaniNo ratings yet
- Ilyas (Hand 2011) - Surgical Approaches To The Distal RadiusDocument10 pagesIlyas (Hand 2011) - Surgical Approaches To The Distal RadiusPaula TrianaNo ratings yet
- Suture Fixation of The Syndesmosis Using Readily Available MaterialsDocument6 pagesSuture Fixation of The Syndesmosis Using Readily Available MaterialsdeparteemyselfNo ratings yet
- Posterior Approach To The RadiusDocument4 pagesPosterior Approach To The RadiusJake sanchezNo ratings yet
- 2021 2.206 机器人辅助双螺钉固定微小移位的舟骨腰部骨折不愈合或延迟愈合,无需植骨Document6 pages2021 2.206 机器人辅助双螺钉固定微小移位的舟骨腰部骨折不愈合或延迟愈合,无需植骨du jiafeiNo ratings yet
- Ibm 1Document7 pagesIbm 1rintanfsNo ratings yet
- Correction of Malunited Intra-Articular Distal Radius Fractures With An Inside-Out Osteotomy TechniqueDocument6 pagesCorrection of Malunited Intra-Articular Distal Radius Fractures With An Inside-Out Osteotomy TechniqueComunicación PiñalNo ratings yet
- Anterior Anterolateral Posterior App Advantages DisadvantagesDocument8 pagesAnterior Anterolateral Posterior App Advantages Disadvantagesmuhammad bayu wicaksonoNo ratings yet
- Green 2013Document4 pagesGreen 2013Angel GutierrezNo ratings yet
- Sicotj 1 14Document5 pagesSicotj 1 14Igor MoraisNo ratings yet
- Completely Thoracoscopic Surgical StabilizationDocument9 pagesCompletely Thoracoscopic Surgical Stabilizationduke3443No ratings yet
- The Pins and Rubbers Traction System FOR Treatment of Comminuted Intraarticular Fractures and Fracture-Dislocations in The HandDocument10 pagesThe Pins and Rubbers Traction System FOR Treatment of Comminuted Intraarticular Fractures and Fracture-Dislocations in The HandAzmi FarhadiNo ratings yet
- Interdigital Approach To Trigger Finger Injection Using Ultrasound GuidanceDocument3 pagesInterdigital Approach To Trigger Finger Injection Using Ultrasound GuidanceputriNo ratings yet
- Ulnar Shortening Versus Distal Radius Corrective Osteotomy in The Management of Ulnar Impaction After Distal Radius MalunionDocument8 pagesUlnar Shortening Versus Distal Radius Corrective Osteotomy in The Management of Ulnar Impaction After Distal Radius MalunionJuan GomezNo ratings yet
- Li 2018Document6 pagesLi 2018Lorena ValderramaNo ratings yet
- Cuadricepsplastia MipiDocument5 pagesCuadricepsplastia MipiVictor HernandezNo ratings yet
- 1 s2.0 S2210261217304431 MainDocument4 pages1 s2.0 S2210261217304431 MainChristopher BermeoNo ratings yet
- Orbay 2016Document6 pagesOrbay 2016Teja Laksana NukanaNo ratings yet
- Muscle-Splitting Posterolateral Thoracotomy: A Novel TechniqueDocument5 pagesMuscle-Splitting Posterolateral Thoracotomy: A Novel TechniqueRizky Angga PNo ratings yet
- 4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaDocument6 pages4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaProfesseur Christian DumontierNo ratings yet
- Dislocation of The Interphalangeal Joint of The Great Toe: Is Percutaneous Reduction of An Incarcerated Sesamoid An Option?Document4 pagesDislocation of The Interphalangeal Joint of The Great Toe: Is Percutaneous Reduction of An Incarcerated Sesamoid An Option?Yariel AraujoNo ratings yet
- Injertos en RinoDocument9 pagesInjertos en RinoDanisse RoaNo ratings yet
- Retromandibular Approach JournalDocument4 pagesRetromandibular Approach JournalAldo AguilarNo ratings yet
- Indications, Surgical Approach, Reduction, and Stabilization Techniques of Distal Radius FracturesDocument11 pagesIndications, Surgical Approach, Reduction, and Stabilization Techniques of Distal Radius FracturesSylvinho46No ratings yet
- 10 1016@j Jhsa 2019 03 014Document6 pages10 1016@j Jhsa 2019 03 014Deborah SalinasNo ratings yet
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- Endoskopik 2.brankialDocument5 pagesEndoskopik 2.brankialDogukan DemirNo ratings yet
- Modified Incision For Maxillectomy: Our ExperienceDocument4 pagesModified Incision For Maxillectomy: Our Experiencedarmayanti ibnuNo ratings yet
- Functional Outcomes of Nonunion Scaphoid Fracture Treated by PDFDocument6 pagesFunctional Outcomes of Nonunion Scaphoid Fracture Treated by PDFHazorthoNo ratings yet
- Rao 2017Document2 pagesRao 2017Guma KipaNo ratings yet
- 2021 - Chronic Isolated Radial Head DislocationDocument9 pages2021 - Chronic Isolated Radial Head Dislocationjuan pablo aguirreNo ratings yet
- Flexible 3D Laparoscopic Assisted Reduction andDocument9 pagesFlexible 3D Laparoscopic Assisted Reduction andgevowo3277No ratings yet
- Tibial Fractures Useful Plastering Technique: MethodDocument4 pagesTibial Fractures Useful Plastering Technique: MethodgregraynerNo ratings yet
- 2016 Article 9341 PDFDocument8 pages2016 Article 9341 PDFJulenda CintarinovaNo ratings yet
- Radial Forearm Free FlapDocument54 pagesRadial Forearm Free FlapWakilAhmadNo ratings yet
- JC - Endoscopic Techniques in OralDocument33 pagesJC - Endoscopic Techniques in OralNarla SusheelNo ratings yet
- Jaw Surgery: Robert M. Menard, Nikhil K. DesaiDocument10 pagesJaw Surgery: Robert M. Menard, Nikhil K. DesaiAlain AguirreNo ratings yet
- Stav SoucasnyDocument14 pagesStav SoucasnyTommysNo ratings yet
- Endoscopic Transforaminal Discectomy For An Extruded Lumbar Disc HerniationDocument6 pagesEndoscopic Transforaminal Discectomy For An Extruded Lumbar Disc HerniationjuanguapoNo ratings yet
- Acute Compression and Lengthening by The Ilizarov 2006Document7 pagesAcute Compression and Lengthening by The Ilizarov 2006aymanNo ratings yet
- Boyd Approach To ElbowDocument4 pagesBoyd Approach To ElbowGiulio PriftiNo ratings yet
- The Composite Spreader FlapDocument11 pagesThe Composite Spreader FlapameliNo ratings yet
- Current Trends Rhinoplasty Rollin DDocument7 pagesCurrent Trends Rhinoplasty Rollin Dmaxillo.arrasNo ratings yet
- Autogenous Corticocancellous Iliac Bone Graft in Reconstruction of Mandibular Defect: Point of TechniqueDocument4 pagesAutogenous Corticocancellous Iliac Bone Graft in Reconstruction of Mandibular Defect: Point of TechniquekumerrajandrNo ratings yet
- InterLaminar Window DescriptionDocument6 pagesInterLaminar Window DescriptionTiger PowerNo ratings yet
- 223654-Article Text-546414-1-10-20220403Document6 pages223654-Article Text-546414-1-10-20220403Christopher Freddy Bermeo RiveraNo ratings yet
- Evaluation of Functional Outcome of Subtrochanteric Fracture of Femur Treated Surgically With Long Proximal Femoral NailDocument5 pagesEvaluation of Functional Outcome of Subtrochanteric Fracture of Femur Treated Surgically With Long Proximal Femoral NailPradeepa GNo ratings yet
- 1 s2.0 S1010518216303237 MainDocument7 pages1 s2.0 S1010518216303237 MainoscarNo ratings yet
- Hakan 2007 Extended Lateral Supramalleolar Flap For Very Distal Foot Coverage A Case With Arteriovenous MalformationDocument4 pagesHakan 2007 Extended Lateral Supramalleolar Flap For Very Distal Foot Coverage A Case With Arteriovenous MalformationThach Nguyen NgocNo ratings yet
- Frenectomy1 PDFDocument5 pagesFrenectomy1 PDFEdi NugrohoNo ratings yet
- Patella Osteotomy A New Approach For Complex Trauma Around The KneeDocument5 pagesPatella Osteotomy A New Approach For Complex Trauma Around The KneeToño Solano NogueraNo ratings yet
- Arthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalDocument6 pagesArthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalMoustafa MohamedNo ratings yet
- Full Endoscopic Bilateral Over The Top Decompression in LumbarDocument6 pagesFull Endoscopic Bilateral Over The Top Decompression in Lumbarckilincer2No ratings yet
- Acta Orthopaedica Et Traumatologica TurcicaDocument5 pagesActa Orthopaedica Et Traumatologica TurcicaTeja Laksana NukanaNo ratings yet
- Orbay 2016Document6 pagesOrbay 2016Teja Laksana NukanaNo ratings yet
- Approach To Fingertip Injuries: Patricia Martin-Playa,, Anthony FooDocument9 pagesApproach To Fingertip Injuries: Patricia Martin-Playa,, Anthony FooTeja Laksana NukanaNo ratings yet
- Dorsal and Volar Surgical Approaches To The Metacarpophalangeal Joint: A Comparative Anatomic StudyDocument6 pagesDorsal and Volar Surgical Approaches To The Metacarpophalangeal Joint: A Comparative Anatomic StudyTeja Laksana NukanaNo ratings yet
- Michel 2020Document13 pagesMichel 2020Teja Laksana NukanaNo ratings yet
- The Direct Midlateral Approach With Lateral Enlargement of The Pulley System For Repair of Flexor Tendons in FingersDocument6 pagesThe Direct Midlateral Approach With Lateral Enlargement of The Pulley System For Repair of Flexor Tendons in FingersTeja Laksana NukanaNo ratings yet
- Oligoanalgesia in Adult Colles Fracture Patients Admitted To The Emergency DepartmentDocument18 pagesOligoanalgesia in Adult Colles Fracture Patients Admitted To The Emergency DepartmentTeja Laksana NukanaNo ratings yet
- Eduardo 2020Document11 pagesEduardo 2020Teja Laksana NukanaNo ratings yet
- Diagnosisand Managementofacute Scaphoidfractures: M. Diya Sabbagh,, Mohamed Morsy,, Steven L. MoranDocument11 pagesDiagnosisand Managementofacute Scaphoidfractures: M. Diya Sabbagh,, Mohamed Morsy,, Steven L. MoranTeja Laksana NukanaNo ratings yet
- Glickel 2019Document5 pagesGlickel 2019Teja Laksana NukanaNo ratings yet
- Dashe 2019Document5 pagesDashe 2019Teja Laksana NukanaNo ratings yet
- Ilich 2000Document7 pagesIlich 2000Teja Laksana NukanaNo ratings yet
- Incidence of An Anomalous Course of The Palmar Cutaneous Branch of The Median Nerve During Volar Plate Fixation of Distal Radius FracturesDocument4 pagesIncidence of An Anomalous Course of The Palmar Cutaneous Branch of The Median Nerve During Volar Plate Fixation of Distal Radius FracturesTeja Laksana NukanaNo ratings yet
- Surgery For Trigger Finger (Review) : CochraneDocument157 pagesSurgery For Trigger Finger (Review) : CochraneTeja Laksana NukanaNo ratings yet
- Aliuskevicius 2019Document10 pagesAliuskevicius 2019Teja Laksana NukanaNo ratings yet
- Complexflexorandextensor Tendoninjuries: Matthew J. Carty,, Philip E. BlazarDocument11 pagesComplexflexorandextensor Tendoninjuries: Matthew J. Carty,, Philip E. BlazarTeja Laksana NukanaNo ratings yet
- Review Article Spontaneous Flexor Tendon Ruptures of The Hand: Case Series and Review of The LiteratureDocument11 pagesReview Article Spontaneous Flexor Tendon Ruptures of The Hand: Case Series and Review of The LiteratureTeja Laksana NukanaNo ratings yet
- Fracturesofthecarpal Bones: Brian M. Christie,, Brett F. MichelottiDocument9 pagesFracturesofthecarpal Bones: Brian M. Christie,, Brett F. MichelottiTeja Laksana NukanaNo ratings yet
- Two Casting Methods Compared in Patients With Colles' Fracture: A Pragmatic, Randomized Controlled TrialDocument12 pagesTwo Casting Methods Compared in Patients With Colles' Fracture: A Pragmatic, Randomized Controlled TrialTeja Laksana NukanaNo ratings yet
- Evidence-Based Management of Patients With Colles' Fractures in Emergency Departments: A Case-Based Critical ReflectionDocument7 pagesEvidence-Based Management of Patients With Colles' Fractures in Emergency Departments: A Case-Based Critical ReflectionTeja Laksana NukanaNo ratings yet
- Jurnal AsliDocument11 pagesJurnal AsliTeja Laksana NukanaNo ratings yet
- WJGS 13 574Document12 pagesWJGS 13 574Teja Laksana NukanaNo ratings yet
- Zaid 2013Document3 pagesZaid 2013Teja Laksana NukanaNo ratings yet
- WJGS 13 164Document13 pagesWJGS 13 164Teja Laksana NukanaNo ratings yet
- Pih 2020Document6 pagesPih 2020Teja Laksana NukanaNo ratings yet
- WJGS-13-330 2Document11 pagesWJGS-13-330 2Teja Laksana NukanaNo ratings yet
- Exposure To Air During Surgery Inhibits Cellular: Activity in Flexor TendonsDocument4 pagesExposure To Air During Surgery Inhibits Cellular: Activity in Flexor TendonsTeja Laksana NukanaNo ratings yet
- Scrotal Abscess As The First Symptom of Fatal Necrotizing PancreatitisDocument4 pagesScrotal Abscess As The First Symptom of Fatal Necrotizing PancreatitisTeja Laksana NukanaNo ratings yet
- College of Physical and Respiratory Therapy S.Y. 2016-2017: Bernardo Tayaban JR., PTRP Maverick Kaypee Colet, PTRPDocument7 pagesCollege of Physical and Respiratory Therapy S.Y. 2016-2017: Bernardo Tayaban JR., PTRP Maverick Kaypee Colet, PTRPVanessa Yvonne GurtizaNo ratings yet
- WORKSHEET 11.1 Locomotion and Support in Humans and AnimalsDocument6 pagesWORKSHEET 11.1 Locomotion and Support in Humans and Animalsmiedsassin67% (3)
- Fractures of The Distal End of The Radius Treated by Internal Fixation and Early Function. A Preliminary Report of 20 CasesDocument6 pagesFractures of The Distal End of The Radius Treated by Internal Fixation and Early Function. A Preliminary Report of 20 Casessanjay chhawraNo ratings yet
- Lateral Condylar Fracture in ChildrenDocument19 pagesLateral Condylar Fracture in ChildrenMuhammed Muzzammil SanganiNo ratings yet
- SKELETAL SYSTEM-WPS OfficeDocument7 pagesSKELETAL SYSTEM-WPS OfficeAlan Gandidze MotifNo ratings yet
- Bone Development and GrowthDocument21 pagesBone Development and GrowthRania ThiniNo ratings yet
- Anatomi Terapan Vertebra Thorakal Dan Rongga ThoraksDocument43 pagesAnatomi Terapan Vertebra Thorakal Dan Rongga ThoraksGilda PutriNo ratings yet
- Anatomy & Physiology: Essentials ofDocument93 pagesAnatomy & Physiology: Essentials ofRamzen Raphael DomingoNo ratings yet
- Anatomy Skeletal Tissue - Chap 5Document30 pagesAnatomy Skeletal Tissue - Chap 5pancit cantonNo ratings yet
- Anatomy Final All Questions (New)Document175 pagesAnatomy Final All Questions (New)Sevval OzcelikNo ratings yet
- Fracture ReportDocument19 pagesFracture Reporteros_mimiNo ratings yet
- Prof. Dr. Hazem Abd El-Azeem Professor of Orthopaedic Surgery Cairo UniversityDocument47 pagesProf. Dr. Hazem Abd El-Azeem Professor of Orthopaedic Surgery Cairo UniversitytarikeopsNo ratings yet
- Anatomy and Physiology of Facial BonesDocument12 pagesAnatomy and Physiology of Facial BonesAubrey Unique Evangelista100% (2)
- Legg Calvé Perthes Disease 1Document66 pagesLegg Calvé Perthes Disease 1Vignesh WaranNo ratings yet
- KP 2Document16 pagesKP 2niaNo ratings yet
- Extremitas SuperiorDocument39 pagesExtremitas SuperiorLia NurNo ratings yet
- Anatomy Note PDFDocument67 pagesAnatomy Note PDFanon_251667476No ratings yet
- Bone Anatomy Viewer GameDocument1 pageBone Anatomy Viewer GameAngelica DiolataNo ratings yet
- ChondromaDocument20 pagesChondromapkalikinkarojhaNo ratings yet
- Musculoskeletal SystemDocument46 pagesMusculoskeletal Systemapi-87967494100% (1)
- Biomechanics and Pathomechanics of Elbow JointDocument44 pagesBiomechanics and Pathomechanics of Elbow JointAshwini BajajNo ratings yet
- 02 The Nose and The Associated StructuresDocument72 pages02 The Nose and The Associated Structuresmalaths757No ratings yet
- 1-Biomechanics of Cervical Spine StructureDocument22 pages1-Biomechanics of Cervical Spine Structuresayyed alauddinNo ratings yet
- Bone Age Estimation Using Clavicle BoneDocument8 pagesBone Age Estimation Using Clavicle Boneamapink94No ratings yet
- Muscles of The ScapulaDocument6 pagesMuscles of The ScapulaAndika Anjani AgustinNo ratings yet
- Bhatia MCQ Oral Max SurgeryDocument49 pagesBhatia MCQ Oral Max SurgeryAhmed Marmash100% (1)
- Caldwell Luc - Radical Antrostomy - Procedure Canine Fossa and Inferior Meatal Puncture and Inferior Meatal AntrostomyDocument13 pagesCaldwell Luc - Radical Antrostomy - Procedure Canine Fossa and Inferior Meatal Puncture and Inferior Meatal AntrostomyAlexi Chávez EchevarríaNo ratings yet
- The HandDocument4 pagesThe HandRoland Garcia Pelagio Jr.No ratings yet
- Chapter 14 SkeletonDocument6 pagesChapter 14 SkeletonJian Leong ThoNo ratings yet
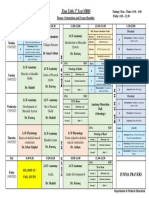
- Timetable 1st Year MBBS MSK Module Week 2Document1 pageTimetable 1st Year MBBS MSK Module Week 2UZAIR KHANNo ratings yet