You might also like
- Approach To FatigueDocument27 pagesApproach To FatigueBasil HussamNo ratings yet
- Fatigue & Tiredness: Done By: Mohammed Z. SharadqahDocument29 pagesFatigue & Tiredness: Done By: Mohammed Z. SharadqahMohammed SharadqahNo ratings yet
- Chronic Fatigue Syndrome: Ashton JeppesenDocument30 pagesChronic Fatigue Syndrome: Ashton Jeppesenmandala22No ratings yet
- ME/CFS Primer For Clinical PractitionersDocument42 pagesME/CFS Primer For Clinical PractitionersFernando GómezNo ratings yet
- Chronic Fatigue Syndrome: Diagnosis and TreatmentDocument6 pagesChronic Fatigue Syndrome: Diagnosis and TreatmentHitesh VermaNo ratings yet
- JCSM 11 9 1029 PDFDocument10 pagesJCSM 11 9 1029 PDFNonoNo ratings yet
- Adrenal Fatigue Solution: Powerful Methods to Boost Your Energy, Improve Metabolism, And Stimulate Your HormonesFrom EverandAdrenal Fatigue Solution: Powerful Methods to Boost Your Energy, Improve Metabolism, And Stimulate Your HormonesNo ratings yet
- FatigueDocument26 pagesFatigueAbdulbari AL-GhamdiNo ratings yet
- Chronic Fatigue Syndrome: An Overview of Diagnosis and TreatmentDocument65 pagesChronic Fatigue Syndrome: An Overview of Diagnosis and TreatmentDavid_Waltos_2571No ratings yet
- PBL 1-1 CFSDocument54 pagesPBL 1-1 CFSsylvia haryantoNo ratings yet
- All My Test Results are Normal: A Smart Guide to Testing for Chronic Fatigue SyndromeFrom EverandAll My Test Results are Normal: A Smart Guide to Testing for Chronic Fatigue SyndromeRating: 2.5 out of 5 stars2.5/5 (2)
- Chronic Fatigue Syndrome: - A Toolkit For ProvidersDocument17 pagesChronic Fatigue Syndrome: - A Toolkit For ProvidersNoorAkNo ratings yet
- The Vitamin Cure for Chronic Fatigue Syndrome: How to Prevent and Treat Chronic Fatigue Syndrome Using Safe and Effective Natural TherapiesFrom EverandThe Vitamin Cure for Chronic Fatigue Syndrome: How to Prevent and Treat Chronic Fatigue Syndrome Using Safe and Effective Natural TherapiesNo ratings yet
- Clinical Research Methods: Interventional Clinical ResearchDocument56 pagesClinical Research Methods: Interventional Clinical ResearchNarayana NaveenkumarNo ratings yet
- Chronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsFrom EverandChronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsNo ratings yet
- Physical Examination in Psychiatric Practice: Gill GardenDocument8 pagesPhysical Examination in Psychiatric Practice: Gill Gardenyeremias setyawanNo ratings yet
- Physical Examination Skills Vital for PsychiatristsDocument8 pagesPhysical Examination Skills Vital for PsychiatristsDita Mega UtamiNo ratings yet
- Persisten Fatigue Stephen2008Document10 pagesPersisten Fatigue Stephen2008abraham rumayaraNo ratings yet
- Chart Stimulated Recall SlidesDocument40 pagesChart Stimulated Recall Slidesnpr00No ratings yet
- Pre Lab Work Health AssessmentDocument11 pagesPre Lab Work Health AssessmentSarah Jane VasquezNo ratings yet
- Edmonds M. Et Al. Exercise Therapy For Chronic Fatigue Syndrome. Cochrane Database Syst Rev 2004 3 CD003200Document22 pagesEdmonds M. Et Al. Exercise Therapy For Chronic Fatigue Syndrome. Cochrane Database Syst Rev 2004 3 CD003200Riana Pasca RoshianNo ratings yet
- Pharma To Therapy For CFSDocument10 pagesPharma To Therapy For CFSbaxterleo100% (1)
- Family Medicine - General Practice MEQ 2006Document6 pagesFamily Medicine - General Practice MEQ 2006jermie22100% (1)
- Skills: Rational Test OrderingDocument4 pagesSkills: Rational Test OrderingJanNo ratings yet
- Fatigue: Done By: Nancy Ghishan Amr LahlouhDocument24 pagesFatigue: Done By: Nancy Ghishan Amr LahlouhazmimustafaNo ratings yet
- A Critical Examination of The Homeopathic Treatment of Chronic Fatigue SyndromeDocument18 pagesA Critical Examination of The Homeopathic Treatment of Chronic Fatigue SyndromeceliastNo ratings yet
- Somatoform Autonomic DysfunctionDocument36 pagesSomatoform Autonomic DysfunctionSuhana ShresthaNo ratings yet
- Functional Medicine OverviewDocument28 pagesFunctional Medicine Overviewmdesdoc50% (4)
- Running Head: Polysomnography 1: Polysomnography Questions Name Institutional AffiliationDocument8 pagesRunning Head: Polysomnography 1: Polysomnography Questions Name Institutional AffiliationRobert MariasiNo ratings yet
- The Perrin Technique 2nd edition: How to diagnose and treat chronic fatigue syndrome/ME and fibromyalgia via the lymphatic drainage of the brainFrom EverandThe Perrin Technique 2nd edition: How to diagnose and treat chronic fatigue syndrome/ME and fibromyalgia via the lymphatic drainage of the brainRating: 5 out of 5 stars5/5 (1)
- Psychiatry Practice BoostersFrom EverandPsychiatry Practice BoostersJesse KoskeyNo ratings yet
- A Case Study On MigraineDocument35 pagesA Case Study On MigraineRitu ShewaniNo ratings yet
- Exercise Physiology for the Pediatric and Congenital CardiologistFrom EverandExercise Physiology for the Pediatric and Congenital CardiologistNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 12: NeurologyFrom EverandComplementary and Alternative Medical Lab Testing Part 12: NeurologyNo ratings yet
- Complex Febrile Seizures - Dr. Albert JamesDocument4 pagesComplex Febrile Seizures - Dr. Albert JamesRohit BharadwajNo ratings yet
- Effects of Stretching On Menopausal and Depressive Symptoms in Middle-Aged Women: A Randomized Controlled TrialDocument6 pagesEffects of Stretching On Menopausal and Depressive Symptoms in Middle-Aged Women: A Randomized Controlled TrialGorkaBuesaNo ratings yet
- Overview: Mind-Body Medicine: The Biopsychosocial ModelDocument27 pagesOverview: Mind-Body Medicine: The Biopsychosocial ModelGovind Chandra DwivediNo ratings yet
- 9-Dalia Jan 2008Document9 pages9-Dalia Jan 2008Menna Tesfaye MigbarNo ratings yet
- Cognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationFrom EverandCognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationMark MuseNo ratings yet
- Chronische Mudigkeit 2020 Klinghardt MüdigkeitDocument99 pagesChronische Mudigkeit 2020 Klinghardt Müdigkeitzim1dsgvo.ruNo ratings yet
- Exercise and DepressionDocument5 pagesExercise and DepressionDumitrescu TinaNo ratings yet
- Anti-Aging Therapeutics Volume XIIIFrom EverandAnti-Aging Therapeutics Volume XIIINo ratings yet
- UntitledDocument46 pagesUntitledapi-257817850No ratings yet
- Differential Diagnosis and Clinical Decision MakingDocument26 pagesDifferential Diagnosis and Clinical Decision MakingbkdfiesefllNo ratings yet
- Returning to School After Concussion: A Case StudyDocument6 pagesReturning to School After Concussion: A Case StudyhimsumraniNo ratings yet
- Management of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesDocument10 pagesManagement of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesArizkamhNo ratings yet
- Obstructive Sleep ApneaDocument1 pageObstructive Sleep ApneamurdalinNo ratings yet
- Texila American University: Case Report FormatDocument7 pagesTexila American University: Case Report FormatShahzad AhmadNo ratings yet
- Texila American University: Case Report FormatDocument7 pagesTexila American University: Case Report FormatShahzad AhmadNo ratings yet
- Texila American University: Case Report FormatDocument7 pagesTexila American University: Case Report FormatShahzad AhmadNo ratings yet
- Case Study - Mike Kelly - HTN-Atherosclerosis - STUDENT-1Document11 pagesCase Study - Mike Kelly - HTN-Atherosclerosis - STUDENT-1Chaos simmonsNo ratings yet
- Amc Question Bank ClinicalsDocument36 pagesAmc Question Bank ClinicalsSoumen Dutt100% (1)
- 3. 麻醉前访视Document34 pages3. 麻醉前访视simple livingNo ratings yet
- Otorhinolaryngology: Clinical Characteristics of Patients With Persistent Postural-Perceptual DizzinessDocument7 pagesOtorhinolaryngology: Clinical Characteristics of Patients With Persistent Postural-Perceptual DizzinessFernando SalesNo ratings yet
- Gangguan SomatoformDocument6 pagesGangguan SomatoformCalistaParamithaNo ratings yet
- Complementary Therapies in Clinical PracticeDocument7 pagesComplementary Therapies in Clinical PracticeSalvinia Salvy PrihantaNo ratings yet
- Pediatric Meningitis CaseDocument6 pagesPediatric Meningitis CaseAaron Joshua PobreNo ratings yet
- Integrative Medicine Research: Chang-Gue SonDocument3 pagesIntegrative Medicine Research: Chang-Gue SonCarlos DNo ratings yet
- CMAJ Diagnoses During Follow-Up of Patients Presenting 2009Document5 pagesCMAJ Diagnoses During Follow-Up of Patients Presenting 2009twice againNo ratings yet
- Anti Inflammatory Diets 2015Document9 pagesAnti Inflammatory Diets 2015twice againNo ratings yet
- BMC Family Practice The Differential Diagnosis of Tiredness 2016Document11 pagesBMC Family Practice The Differential Diagnosis of Tiredness 2016twice againNo ratings yet
- Fatigue (CMAJ) PDFDocument3 pagesFatigue (CMAJ) PDFDapot SianiparNo ratings yet
- Ordering Blood Tests For Patients With Unexplained Fatigue in General Practice 2009Document8 pagesOrdering Blood Tests For Patients With Unexplained Fatigue in General Practice 2009twice againNo ratings yet
- Brief and Distinct Empirical Sleepiness and Fatigue Scales 2006Document9 pagesBrief and Distinct Empirical Sleepiness and Fatigue Scales 2006twice againNo ratings yet
- Fellowship Directory (5-4-21)Document32 pagesFellowship Directory (5-4-21)twice againNo ratings yet
- 00000fatigue An Overview PDFDocument7 pages00000fatigue An Overview PDFAlp HatNo ratings yet
- Pediatr Rev - Urine Electrolytes 2011Document4 pagesPediatr Rev - Urine Electrolytes 2011twice againNo ratings yet
- EAGLES Varenicline Bupropion Nicotine PatchDocument14 pagesEAGLES Varenicline Bupropion Nicotine Patchtwice againNo ratings yet
- Conclave BrochureDocument3 pagesConclave BrochureRebekah AngelNo ratings yet
- Cse Cg-Aral PanDocument17 pagesCse Cg-Aral PanJess Devaras100% (1)
- Childhood Cognitive Development StagesDocument5 pagesChildhood Cognitive Development Stagesjohn mwambuNo ratings yet
- CREST Final ReportDocument21 pagesCREST Final ReportDarren KrauseNo ratings yet
- Chapter 11 Hormonal Coordination: 165 MinutesDocument60 pagesChapter 11 Hormonal Coordination: 165 MinutesAviBreezeNo ratings yet
- Chap 26 - Assessing Male Genitalia (Interview Guide)Document3 pagesChap 26 - Assessing Male Genitalia (Interview Guide)Mary Cielo DomagasNo ratings yet
- 2020 Tuition Fee Tables For International StudentsDocument31 pages2020 Tuition Fee Tables For International StudentsMiss PurwantiNo ratings yet
- Why Texting Is Better Than TalkingDocument4 pagesWhy Texting Is Better Than TalkingjhgfhjgkgkNo ratings yet
- Infection Control: The New York RequirementDocument3 pagesInfection Control: The New York RequirementLiezel100% (1)
- Lumi Juice CaseDocument6 pagesLumi Juice CaseIsmael BastidaNo ratings yet
- HsjshsjdhehsjDocument4 pagesHsjshsjdhehsjKimberly ValsoteNo ratings yet
- Umar 2Document3 pagesUmar 2Tufail YaseenNo ratings yet
- NHS FPX 6008 Assessment 4 Lobbying for ChangeDocument6 pagesNHS FPX 6008 Assessment 4 Lobbying for Changejoohnsmith070No ratings yet
- MARIELLE CHUA - (Template) SOAPIE CaseletDocument9 pagesMARIELLE CHUA - (Template) SOAPIE CaseletMarielle Chua100% (1)
- Donning and Doffing PPEDocument4 pagesDonning and Doffing PPEShang DimolNo ratings yet
- Mini-CEX (2013) : Notes of Attention To The Competences Which Are Shown During The mini-CEXDocument1 pageMini-CEX (2013) : Notes of Attention To The Competences Which Are Shown During The mini-CEXJean JeanNo ratings yet
- Measurement Uncertainty According To ISO 19036:2019Document8 pagesMeasurement Uncertainty According To ISO 19036:2019ghadeerNo ratings yet
- Session 3 Creating A Positive Workplace For Employee Mental Health FINALDocument27 pagesSession 3 Creating A Positive Workplace For Employee Mental Health FINALMYRA GONZALESNo ratings yet
- The Outsiders Complete VocabularyDocument4 pagesThe Outsiders Complete VocabularyOsman HuseynliNo ratings yet
- Total Vacancies in All Cadres: Zone Contract ContractDocument14 pagesTotal Vacancies in All Cadres: Zone Contract ContractMadhan MohanNo ratings yet
- How Would You Reconcile The Ad and Disad of GMOsDocument4 pagesHow Would You Reconcile The Ad and Disad of GMOsLianna RodriguezNo ratings yet
- 1.8 Annex 4 - BOPIS DCF FORM 2-BDocument2 pages1.8 Annex 4 - BOPIS DCF FORM 2-Bgulp_burp75% (4)
- Reinforcement TheoryDocument10 pagesReinforcement TheorySana taNo ratings yet
- CHAPTER 4: Modifiable Risk Factors of Lifestyle Diseases: SmokingDocument4 pagesCHAPTER 4: Modifiable Risk Factors of Lifestyle Diseases: SmokingShimah100% (2)
- Quiz1 KeyDocument8 pagesQuiz1 KeyAli KalyarNo ratings yet
- PSORIASISDocument9 pagesPSORIASISDianne BernardoNo ratings yet
- Re Beacon Conference MeetingDocument11 pagesRe Beacon Conference MeetingjohnsherwieNo ratings yet
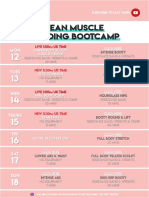
- 26 - LEAN Weekly Guide - On - October 12Document15 pages26 - LEAN Weekly Guide - On - October 12Andrea CsillaNo ratings yet
- Case Presentation/ Analysis - Hyperkalemia: ContosoDocument48 pagesCase Presentation/ Analysis - Hyperkalemia: Contosokesia abañoNo ratings yet
- Assignment Four Developments in Equine Care EssayDocument4 pagesAssignment Four Developments in Equine Care EssayEmma WalshNo ratings yet