Professional Documents
Culture Documents
Lorenzo Vanini 2 PDF Free
Lorenzo Vanini 2 PDF Free
Uploaded by
NonoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Lorenzo Vanini 2 PDF Free
Lorenzo Vanini 2 PDF Free
Uploaded by
NonoCopyright:
Available Formats
e n e fit:
e m ber B 100
A A CD Mee page
New rn CE—s
Ea
Conservative Composite
Restorations that Mimic Nature
A Step-by-Step Anatomical Stratification Technique
Lorenzo Vanini, DDS, MD
Learning Objectives:
After reading this article, the participant
should be able to:
1. Understand the author’s theory of the five
dimensions of color and understand the im-
portance of shape and color in dentistry.
2. Learn how to achieve a predictable compos-
ite restoration following the anatomical or
natural stratification of the tooth.
3. Understand the refraction index phenom-
enon, which results in reproducing natural
enamel and invisible margins.
80 Fall 2010 • Volume 26 • Number 3
Vanini
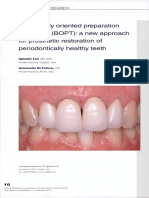
Figure 1: Color determination usually is achieved using shade
guides made with different materials and stratification of the
shade to be used by the dentist.
Abstract Compounding the problem has The Five Color Dimensions
been the absence of precise protocol of Teeth
This article presents the author’s theory and planned management of the bod-
of the five dimensions of color as a basis ies and thicknesses of materials from Color in dentistry usually is defined
for developing esthetic direct composite manufacturers. The conventional color using shade guides based upon the
restorations that mimic natural den- determination systems and techniques 1898 theory of American painter Albert
tition, and describes his step-by-step still used today are based on a chromat- Henry Munsell, which Clark applied
anatomical stratification technique for ic scale more than 80 years old.1 Based to dentistry in 1930.7 According to this
composite placement. By understand- on Munsell’s three dimensions of color, theory, color is composed of three di-
ing the refractive index of composites typical shade guides do not represent mensions: hue, chroma, and value
and analyzing tooth structures, den- the body and thickness of natural tooth (Fig 1). Hue is the basic shade of the
tists can achieve predictable composite anatomy.3 tooth; chroma is the degree of satura-
restorations that replicate the optical tion of the hue; and value represents lu-
properties of natural enamel and den- minosity. The Classic VITA Shade Guide
tin structures.
Color matching is viewed (Vident; Brea, CA) presents four basic
as one of the most hues (e.g., A, B, C, and D) and four
Introduction challenging tasks in chromas for each hue.
Tooth color, however, is actually a
Color matching, one of the key factors
esthetic dentistry. complex culmination of many factors
for determining esthetics, historically resulting from the interaction of enam-
has been fraught with confusion. In the el and dentin with light during the re-
past, clinicians have tried to quantify Materials should serve the clinician, fraction and reflection phenomenon of
tooth color and shade variables with not vice versa. Each composite system light waves. In the enamel area, shorter
various explanations and determina- should be developed based on research waves close to white-blue dominate,
tions. However, no single model has and reproducible, universal techniques while the longer yellow-orange waves
provided an exact solution to the prob- for determining color.4-6 Therefore, to are more evident in the dentin.
lem of matching the color of restorative obtain a predictable esthetic restorative Tooth enamel (Figs 2a & 2b) displays
materials to that of natural dentition.1 result, precise and repeatable clinical the unique light characteristics of reflec-
As a result, color matching is viewed as protocol that begin with analysis of tion, absorption, and transmittance.
one of the most challenging tasks in es- tooth shape and five color dimensions The crystalline structure of the enamel
thetic dentistry.2 are required.1,6 Such analysis will enable prisms allows light to pass freely, while
Additionally, during the past 20 clinicians to realize a stratification the inter-prismatic substance is opaque.
years, dentists frequently have changed technique that incorporates dentin Enamel acts as a translucent system,
materials and techniques. Often they and enamel materials specifically combining partial light transmission
developed their own stratification tech- developed to reproduce the determined and internal light diffusion. The degree
niques that sometimes were completely tooth anatomy. of enamel translucency depends on its
unrelated to the optical properties of thickness, which affects the value (lu-
the restorative material being used. minosity) of the tooth, something that
changes with age.
Journal of Cosmetic Dentistry 81
Figures 2a & 2b: Enamel absorbs and reflects light, filtering
four basic shades: yellow-orange, white, blue, and amber. The
hues of these four shades, or “chromatic chords,” vary among
patients and according to their age.
In young teeth (Fig 3), enamel is thicker and
presents a high density, low translucency, high lu-
minosity (value), and high reflectivity. In old teeth
(Fig 4), enamel is thinner and presents low density,
high translucency, low luminosity (value), and low
reflectivity.
In the tooth area where only enamel is present (i.e.,
incisal edge), the internal light reflection phenome-
non creates the opalescence effect, which typically ap-
pears as blue and amber hues that create the incisal
halo. Frequently, less mineralized areas that appear
white (intensives) are present in the enamel.
Dentin is responsible for the hue and chroma of a
tooth. In natural teeth, the degree of dentin saturation
decreases from the cervical to incisal, and chromatic-
ity increases with aging.3 Dentin also is responsible for
tooth fluorescence. It absorbs the ultraviolet energy
Figure 3: In young teeth, the enamel is thick, dense, with low and diffuses it back as bluish light. Fluorescence re-
translucency, high luminosity (value), and high reflectivity. duces metamerism, the phenomenon in which tooth
color changes depending on the angle and source of
light.
Tooth color, therefore, is the complex result of sev-
eral factors that must be carefully analyzed in order
to understand the unique features that characterize an
individual patient’s teeth. To analyze tooth color, the
author advocates abandoning classical shade guides
and, along with them, customary shade-taking habits
in favor of performing a higher level of tooth color
analysis.1,6 Ultimately the tooth color we see is a func-
tion of the physical properties of dentin and enamel,
and their interaction with light.
The author’s theory of tooth color incorporates a
detailed analysis of each component responsible for
tooth color that can be recorded using a special col-
or chart and subsequently reproduced using specific
Figure 4: In older teeth, the enamel is thin, has low density, materials during the stratification phase. Significant
high translucency, low luminosity (value), and low reflectivity. to this theory is the concept that tooth color is com-
82 Fall 2010 • Volume 26 • Number 3
Figure 5: The five color dimensions in dentistry according to Figure 6: Sample of natural tooth enamel (left) and ENA HRi
the author’s technique. UE2 composite enamel (right). Each sample is 1 mm thick,
showing very similar hue and translucency.
posed of five dimensions. These dimen- appear white. They are classified by four substance) and, therefore, restorative
sions are based on the four main hues shape types: spot, small clouds, snow- composite materials should demon-
that present with different tooth shapes flakes, and horizontal bands.1 strate optical properties similar to those
and intensities, depending on age: of dentin and enamel.1,4-6 Enamel is the
yellow-orange, white, blue, and amber. The speed of light most important structure for this rela-
These four hues, also called “chromat- tionship with light, since it covers the
ic chords,” are responsible for the five
through a material dentin structure similar to a fiber-optic
color dimensions, outlined as follows depends on the system. The translucency and refractive
(Fig 5).1 material’s density. index of composites are very important
and also should closely approximate
1. Chromaticity
It is faster through air those of the natural enamel.
Chromaticity is the hue and chroma of than water. The speed of light through a mate-
the dentin body. The composite used rial depends on the material’s density.
in the author’s stratification technique It is faster through air than water. The
requires only one hue, called UD (Uni- 4. Opalescents refractive index is the ratio of the speed
versal Dentine), and different chromas Opalescents are confined to the incisal of light in vacuum compared to a spe-
(0, 0.5, 1, 2, 3, 4, 5, and 6). In anterior third, the interproximal level, and the cific medium; the wavelength of light
teeth, the chromaticity desaturates from margin where free enamel is located. also affects the refractive index. The
the cervical to the incisal and from the These produce the blue and amber hues more optically compact a medium is,
palatal to buccal, and usually is lower in that create the incisal halo and can ex- the slower the speed of light.
young teeth and higher in old teeth.1,3 hibit different shapes: mammelon, split
mammelon, comb-like, window-like, Considerations For Composite Materials
2. Value or Luminosity and stain-like.1 The refractive index (n) of natural
Value or luminosity is strictly related to enamel is 1.62, while the average refrac-
enamel. The more mineralized and thin 5. Characterizations tive index of composite and ceramic re-
the enamel is, the shinier and lower in Characterizations affect both dentin storative materials is 1.50. The refractive
value it appears, such as in the old tooth and enamel. There are five characteriza- index of glass is 1.52, which means that
biotype. The thicker, more porous, and tions: two in the dentin (mammelon composite and ceramic restorative ma-
more poorly demineralized the enamel and band) and three in the enamel terials have optical properties that are
is, the less translucent and higher in (e.g., margin for young teeth, stain, and more similar to glass than to enamel.
value it appears, such as in the young cracks for adult and old teeth).1 This presents problems when managing
tooth biotype.1 the relationship between translucency
Significance of Refractive and value, because increasing material
3. Intensives Index thickness lowers value (i.e., glass effect),
Intensives occur more frequently in while the behavior of natural enamel is
young tooth biotypes and represent Color results from the relationship be- exactly the opposite.4
hypo-mineralized areas of enamel that tween light and an object (i.e., body/
84 Fall 2010 • Volume 26 • Number 3
Vanini
Figure 7: ENA HRi UE2 enamel samples with increasing thickness over a
sample of UD3 dentin. The ENA HRi enamel, with a refraction index of 1.62,
demonstrates optical behavior similar to natural enamel. Increasing the
thickness also increases the value.
When choosing an enamel compos- enamel and composite enamel) with cording to a different application proto-
ite material, the material should func- the same refractive index. As a result, col than previous composites. A slightly
tion like natural enamel, presenting a there is no deviation in optical prop- thinner layer of similar thickness as the
high translucency and demonstrating erties that would otherwise create the enamel being replaced on the tooth,
the same refractive index.4 When the with no visible margin, is necessary.6
proper index is matched, thicker layers
of the enamel composite will appear
All tooth color Determining Tooth Color
whiter, with high value, high luminos- information should Using the Five Dimensions
ity, and low translucency.4 When ap- be recorded in an
plied more thinly, the enamel com- To properly determine tooth color, den-
posite should appear more translucent,
uncomplicated manner. tists should carefully analyze the tooth
with a low value, low luminosity, and structures (e.g., dentin and enamel)
high translucency.4 Unfortunately, as clinical challenge of a gray line appear- and identify the five color dimensions
the thickness of standard enamel com- ing on the margin.4 Furthermore, when and chromatic chords.1,6 To facilitate
posite layers increases, the percentage of placed for incisal edge restorations, the this process, research has demonstrat-
gray or glass-like effect increases in pro- composite is seamlessly integrated, re- ed that a light with a constant color
portion as well.4 placing the full enamel thickness, with temperature of 5500K is ideal for
no need for dentin composites—unlike shade evaluation (Optilume Trueshade,
Composites With Natural Enamel when using other composite materials Optident; Ilkley, UK) (Fig 9).8 Addi-
Properties (Figs 8a & 8b).4 tionally, the use of digital photography
However, a composite system devel- This composite system also includes is fundamental to the analysis of color
oped by the author includes an enamel universal dentin shades (UD) that are dimensions because it quickly enables
composite that demonstrates a re- available in eight chromatic levels, deeper examination of the tooth on a
fractive index of 1.62 and has optical ranging from Bleach C (UD0) to the computer. Underexposing the photo-
properties very close to those of natu- darker High C (UD6), many of which graph and increasing the contrast al-
ral enamel (HRi Universal Enamels, correspond with the Vita Shade Guide lows better visualization of the color
Micerium S.p.A.; Avegno, Italy) (Fig 6). system.6 Although complex restora- dimensions and increases the am-
Increasing the material’s thickness in- tions may require a basic hue and then ber and blue hues of the incisal halo
creases the value (Fig 7). It is possible the next two darker dentin shades to (Figs 10a & 10b).
with this enamel composite to manage achieve final shading, most restorations
the relationship between translucency can be completed with only one shade Recording Tooth Color/Characterization
and value, as well as the esthetic integra- of this dentin composite.6 Information
tion of the margin, because light passes The unique properties of this com- All tooth color information should be
through the two structures (i.e., natural posite material require placement ac- recorded in an uncomplicated manner.
Journal of Cosmetic Dentistry 85
Figures 8a & 8b: Incisal margin fracture. The free enamel is restored using only HRi composite enamel UE2, achieving an
excellent esthetic integration.
To properly determine
tooth color, dentists
should carefully analyze
the tooth structures...
and identify the five
color dimensions and
chromatic chords.
Figure 9: Direct color determination using a special light with
a color temperature of 5.500 K.
Figures 10a & 10b: The color dimension and the amber and blue hues of the incisal halo are better visualized by underexposing
the image and increasing the contrast.
86 Fall 2010 • Volume 26 • Number 3
predicts recurring dimensions for shape
and chromatic saturation.
It is important to note that color
chart completion should be undertak-
en prior to restorative procedures and
consulted throughout the stratification
process.1 Once a tooth is dehydrated,
this natural tooth color information
is lost.1,9
Documenting Dimensions of Tooth Color
The first tooth color dimension to be
determined is the basic chromaticity
(BC) (Fig 13), which is derived from
the mean value of the dentin body
chromaticities and should be identified
on the middle third of the tooth using a
Figure 11: Front of the author’s color chart. shade guide made from the same com-
posite material to be used for the strati-
fication. The basic chromaticity should
be recorded on the left side of the chart,
while the dentin composites needed
should be indicated on the right.
Each biotype predicts three basic
chromaticities: two pure and one hy-
brid. The young biotype displays chro-
maticity from one to two (1-1,5-2); the
adult from two to three (2-2,5-3); and
the elderly from three to four (3-3,5-4).
The shape of the dentin body and the
mammelon contour to be reproduced
also must be defined.
The second dimension to be deter-
mined is the value or luminosity of the
enamel (Fig 14), which will be high in
the young biotype (3), medium in the
adult (2), and low in the elderly (1).
Each of these groups expresses diverse
density, translucency, and reflectivity.1
This evaluation can be performed by
Figure 12: Back of the author’s color chart. taking a black-and-white photograph.
To determine intensives, opales-
cents, and characterizations, the pho-
For this purpose, the author developed two blue tooth-shaped spaces. The five tograph is compared to the back of
a specific color-mapping chart for re- color dimensions are indicated on the the color chart, and it is helpful to
searching and identifying the five color left, while the identification initials of analyze the image underexposed with
dimensions and specific materials to the composite system materials (i.e., high contrast.
be used to achieve the required effects.1 enamel, dentin) to be used to repro- Intensives (Fig 15) are present pri-
The color chart represents the scheme duce the chromatic chords of the color marily in the young biotype, where
for the restoration, and its proper com- dimensions are indicated on the right. types 1 (spot) and 3 (snowflakes)
pletion is fundamental for correct re- The back of the chart (Fig 12) lists the are usually seen. Adult and elderly
storative results. classification of intensives, opalescents, biotypes more commonly exhibit in-
The front of the chart (Fig 11) out- and characterizations. Each dimension tensive types 2 (small clouds) and 4
lines patient details and also includes refers to age biotypes, and each biotype (horizontal bands).
88 Fall 2010 • Volume 26 • Number 3
Vanini
Figure 13: When studying tooth chromaticity, it is important to
evaluate the dentin body shape and mammelon contours in
order to reproduce them during stratification.
Figure 14: Taking a black-and-white photograph can be helpful Figure 15: Intensives are represented by opaque white spots,
when studying the value. stains, or bands.
Figure 16: It is very important to evaluate the shape and size of Figure 17: The mammelon and incisal margin characterizations
the incisal in order to reproduce the incisal third in represent the natural frame of the incisal halo.
a natural way.
Journal of Cosmetic Dentistry 89
Figure 18: The filled-in color chart guides the project to build up a correct stratification.
Opalescents (Fig 16) in the young tion.1 Stratification, or incremental palatal to buccal, in a harmonious
biotype appear as gray-blue hues of layering, requires a complex under- and modulated way; exhibits contrast
Types 1 (mammelon) and 2 (split mam- standing of the internal structures of in the incisal area between the dentin
melon); in the adult as gray-blue hues the teeth (i.e., enamel, dentin) and their body, free enamel, and darkness of the
of Types 3 (comb-like) and 4 (window- morphology.5,6 mouth; and diffuses light inside the
like); and in the elderly as amber hues The author’s anatomic stratification tooth, imparting a three-dimensional
of Type 5 (stain-like). technique imitates the tooth anatomy, effect to the restoration.
The characterizations mostly pres- restoring enamel and dentin in their
ent (Fig 17) in the young biotype are respective locations and thicknesses Wax-Up and Matrix Guide
the mammelons (Type 1), which can For Class IV restorations, the use of a
appear white or amber, thus creating a silicone matrix/stent is advised to en-
clear-cut boundary with the opalescents; Anatomic stratification sure the correct anatomic position of
and the incisal margin (Type 3), which involves the the palatal/lingual enamel wall, and to
is emphasized by a white or amber line. support the enamel body application.10
In the elderly biotype, the characteriza-
reproduction of dentin The silicone matrix can be provided by
tions seen are one or more horizontal and enamel tissues to a laboratory from the wax-up or created
bands with a whitish or amber tonality the proper thickness directly in the mouth using a medium-
that extend into the interproximal ar- viscosity silicone and temporary restor-
eas (Type 2); amber or brown stain-like
and position. ative, then shaped and adjusted with
characterization (Type 4) at the incisal burs (Figs 19a-20b). Once the silicone
third; and crack of the enamel (Type 5) to achieve a light-composite-color re- has hardened, the stent is removed and
produced by brown pigmented fissures lationship similar to natural tooth adjusted to fit perfectly to the teeth and
or white opaque cracks. structure. This is accomplished by pre- buccal wall corresponding to the affect-
cisely planning the documented resto- ed tooth, then removed.
Anatomic Stratification and ration of the palatal and interproximal
Composites enamel, the dentin body, and the Isolation, Preparation, and Adhesive
buccal enamel. Protocol
Anatomic stratification involves the The composite stratification is guid- Prior to initiating the stratification tech-
reproduction of dentin and enamel ed by the color chart, which must be nique, the area should be cleaned with
tissues to the proper thickness and po- completed with the characteristics of a fluoride-free prophylaxis paste and
sition.1,5,6 During this process, it also is tooth color dimension prior to initiat- isolation achieved with a rubber dam.
necessary to consider the proteinaceous ing restorative procedures (Fig 18). This For interproximal restorations, a trans-
layer between dentin and enamel that will ensure that the anatomic stratifica- parent matrix is required.
is responsible for the internal diffusion tion demonstrates desaturation of the For Class IV restorations, the ideal
of light and luminosity of the restora- hue from cervical to incisal, and from margin preparation includes a 90° butt
90 Fall 2010 • Volume 26 • Number 3
Vanini
Figures 19a & 19b: View of the model and wax-up.
Figures 20a & 20b: Impression and silicone stents will be used to build up the palatal wall. The buccal part of the stent is
removed to access the cavity and stratify the enamel.
margin on the palatal and interproxi- A thin coat of adhesive bonding Curing should be completed on all
mal margins, and a short chamfer in agent (ENA Bond) is applied to the sides of the stratification for 40 seconds
the buccal margin. The margin is first preparations, down to the margins, and for each 1 mm to 1.5 mm layer. The
prepared using a coarse-grain diamond then light-cured for 40 seconds. If us- light-curing tip should be kept as close
bur, ball-shaped for the chamfer, and ing ENA Bond, a second coat of mate- to the restoration as possible to ensure
cylindrical for the butt margin. The mar- rial should be applied and cured.11 Care a thorough cure. It also is advisable to
gin is finished using the same burs with should be taken to not contaminate turn off the overhead light or not have
fine grain and, afterwards, polished us- the oxygen-inhibiting layer to ensure a it placed directly overhead to prevent
ing a silicone point, since the smooth strong bond to the composite.12 uncontrolled curing.
surface facilitates flow of the adhesive, Using an acetate matrix and a wedge,
as well as composite adaptation on the Composite Application restore the interproximal walls us-
margin (Figs 21a & 21b). Remove the selected composite from ing the same enamel body compos-
The preparations are etched using the syringe and warm to 39°C with a ite that was placed for the palatal wall
a 35% to 38% phosphoric acid (ENA heating container.5 Place the stent in the (Fig 22). Once these two steps have
Etch, Micerium S.p.A.) for 15 to 30 sec- mouth, and begin the Class IV stratifi- been completed, the complex cavity
onds for enamel and vital dentin. For cation by applying the palatal/lingual is transformed into a simple shell, the
sclerotic dentin, 1 minute is necessary, enamel layer. It should be applied in a shape and thickness of which should be
and root non-vital dentin (for post- thickness that approximates that of the verified and eventually corrected prior
adhesive cementation) requires 1.5 natural enamel being replaced, avoid- to continuing with the restoration. The
minutes. The etched surface should be ing the interproximal areas. The stent is volumes to be filled are now evident,
cleaned and dried with oil-free air, leav- used to verify adaptation, then removed making it easier to check the areas that
ing a white appearance on the enamel. for light curing. need to be restored.
Journal of Cosmetic Dentistry 91
Figures 21a & 21b: View of the cavity preparation consisting of a buccal mini-chamfer and interproximal and
palatal butt margins.
Figure 22: Palatal and interproximal walls create an enamel
frame on which the dentin body will be placed.
Figure 23: Dentin body and number of composite dentin masses used according to the cavity size.
92 Fall 2010 • Volume 26 • Number 3
Figure 24: Dentin body stratification is completed with three Figure 25: Dentin body mammelons are characterized with a
shades: UD5, UD3, and UD2. Because the basic chromaticity is thin layer of IW.
hybrid (2,5), the first layer used is UD5 instead of UD4 in order
to increase the chromaticity a half point.
Figure 26: Margin characterization is created with IW and OA. Figure 27: Opalescent natural OBN is placed in the
interproximal grooves and between the mammelons.
For the dentin body restoration, the el is applied and creates a desaturation composition of the dentin body with
number of dentin shades needed corre- from cervical to incisal, and from pala- different chromas and the balanced de-
lates to the size of the preparation: one tal to buccal. saturation seen in natural teeth.
dentin body for small, two for medium, Therefore, in a large preparation After building up the dentin body,
and three for large (Fig 23). Each tooth area, the dentin body stratification be- characterizations, intensives, and opal-
exhibits three degrees of chromaticity: gins at the most cervical margin by plac- escents are placed before applying the
high in the cervical third, medium in ing a high saturation dentin composite buccal enamel layer. The most impor-
the middle third, and low at the incisal cervically. Continuing this example, tant characterizations are the mam-
level.3 Therefore, one or more compos- UD4 would be placed and cured, after melons and the margin (Figs 25 & 26),
ites with increasing saturation should which UD3 would be applied to com- which are reproduced using white and
be used to reproduce these chromatici- pletely cover UD4, as well as placed on amber (IW and OA). Following mam-
ties, based on the size of the cavity. For the buccal chamfer, pushed more inci- melon and margin characterization,
example, if the basic chromaticity is sally, and cured. These two layers then create the opalescents using a specific
UD2, the required dentin body com- are completely covered with a layer of body composite (OBN) that is placed
posite would be UD2 for a small cavity; UD2, which also is placed on the cham- between the mammelons and the area
UD2 and UD3 for a medium cavity; and fer and extended to the incisal margin, between the incisal margin and the den-
UD2, UD3, and UD4 for a large cavity. and cured. If mammelons are present, tine body (Fig 27) to produce a natural
Such an approach achieves a strong the vertical grooves should be opened halo. Finally, reproduce the intensives
chromatic nucleus that prevents the loss first to create the halo shape (Fig 24). in the shape determined during the col-
of chromaticity when the buccal enam- This enables creation of a chromatic
94 Fall 2010 • Volume 26 • Number 3
Vanini
Figure 28: Small increments of IWS, an opaque white body Figure 29: A 0.6-mm increment of UE2 completes
composite, create small intensive spots. the restoration.
or mapping by using the white opaque surface reduces plaque deposits and ag- and position of the transition lines (i.e.,
body composites (IWS, IM) (Fig 28). ing of the restoration. Finishing defines angles that define the transition from
It is important to remember that the shape, dimension, and contour of the interproximal margin to the buccal
when applying the different composites the restoration (Figs 30a & 30b), while surface) are fundamental to the esthetic
to build up the dentin body, charac- polishing shines the surfaces, maintain- integration of the restoration.
terization, opalescents, and intensives, ing the texture details achieved during After adjusting the shape, finish the
necessary space must be left to apply the finishing (Figs 30c-30f). surface macro-texture using a medium-
buccal enamel layer, which is thinner in grain diamond or multi-bladed bur to
the cervical area and thicker at the inci- create lobes and grooves. The enamel
sal edge, with a natural vertical contour Polishing imparts brilliance growth lines (micro-texture) are created
that creates the natural tooth shape. The to the restoration surfaces. using the point of a green stone to gen-
stratification technique concludes with tly scratch the surface.
the buccal enamel layer, which must
The ideal way to polish Polishing imparts brilliance to the
be applied to reproduce the transition a restoration is by using restoration surfaces. The ideal way to
lines and draft both the macro-texture diamond pastes and a goat polish a restoration is by using dia-
(i.e., lobes, grooves, and depressions) mond pastes and a goat hair brush,
and micro-texture, using a brush to cre-
hair brush, which will not which will not destroy the macro- and
ate the enamel growth lines (Fig 29). destroy the macro- and micro-texture surface details. Begin pol-
Once the last layer of enamel is cured micro-texture surface ishing with a 3-µ diamond paste, then
and prior to initiating finishing and switch to a 1-µ paste with water spray.
polishing procedures, it is advisable
details. Polish the interproximal walls using
to cover the surface of the restoration abrasive strips with decreasing grain
with a layer of glycerin gel and perform Begin finishing by correcting the and diamond pastes. The final gloss-
an additional cycle of light-curing to shape using medium-grain diamond ing can be achieved using an aluminum
eliminate the oxygen-inhibited lay- burs (e.g., 30 to 40 µ). Finish the verti- oxide paste with a felt disc, working at
er and obtain complete composite cal contour by following the tooth anat- first without water at a very low speed,
polymerization.11 omy, using the bur along three different then increasing the speed but using co-
inclinations, depending on the area of pious water spray and no pressure on
Finishing and Polishing the tooth (e.g., cervical, incisal, or mid- the restoration surface. When the finish-
dle third). Finish the horizontal con- ing and polishing steps are completed,
Finishing and polishing complete the tour by adjusting the shape and length a conservative composite restoration
restoration and are important steps of the incisal edge and corners; finish should be achieved (Fig 31).
in the process because they create the the interproximal internal margin using
ideal relationship between light and abrasive strips; and finish the interprox-
the tooth, which is fundamental to imal external margin using medium-
achieving the desired esthetic result.13 grain diamond burs. This step is very
Furthermore, the finished and polished important because the correct shape
Journal of Cosmetic Dentistry 95
D E F
Figures 30a-30f: Images demonstrating the main phases of finishing and polishing.
96 Fall 2010 • Volume 26 • Number 3
Vanini
Figure 31: View of the restoration after polishing.
Figures 32a & 32b: A well-integrated esthetic restoration should reproduce all five color dimensions in a natural way.
Figures 33a & 33b: Another example of an esthetic restoration using the five dimensions of color.
Journal of Cosmetic Dentistry 97
Examining tooth color
beyond the typical three References
dimensions of color (i.e.,
hue, chroma, and value) 1. Vanini L, Mangani FM. Determination and communication of
color using the five color dimensions of teeth. Pract Proced
enables dentists to create Aesthet Dent. 2001;13(1):19-26.
highly esthetic restorations
that are indistinguishable 2. Ishikawa-Nagai S, Yoshida A, Sakai M, Kristiansen J, Da Sil-
va, JD. Clinical evaluation of perceptibility of color differ-
from natural dentition. ences between natural teeth and all-ceramic crowns. J Dent.
2009;37(Suppl 1):e57-63. Epub 2009 Apr 18.
3. O’Brien WJ, Hemmendinger H, Boenke KM, Linger JB, Groh
Conclusion CL. Color distribution of three regions of extracted human
teeth. Dent Mater. 1997 May;13(3):179-85.
Examining tooth color beyond the typical three
dimensions of color (i.e., hue, chroma, and val- 4. Vanini L. Light and color in anterior composite restorations.
ue) enables dentists to create highly esthetic res- Pract Periodontics Aesthet Dent. 1996 Sep;8(7):673-82.
torations that are indistinguishable from natural
dentition (Figs 32a & 32b, 33a & 33b).1 Still one 5. Vanini L, Mangani F, Klimovskaia O. Conservative restoration
of the most challenging areas in dentistry, color of anterior teeth. Viterbo (Italy): Editing ACME; 2005.
matching direct composite restoratives to natural
teeth for the realization of natural-looking treat- 6. Vanini L. Anatomic stratification technique. Presented at the
ments can be achieved using new determination 26th Annual AACD Scientific Session; Grapevine, TX, April 27,
techniques and placement protocol. This article 2010.
has described the theory of the five dimensions
of color as a basis for developing esthetic direct 7. Clarke EB. Selection of tooth color for the edentulous patient.
composite restorations and presented the details J Am Dent Assoc. 1947 Dec 1;35(11):787-93.
of a predictable direct placement technique.
8. Gokce HS, Piskin B, Ceyhan D, Gokce SM, Arisan V. Shade
matching performance of normal and color vision-deficient
dental professionals with standard daylight and tungsten il-
luminants. J Prosthet Dent. 2010 Mar;103(3):139-47.
9. Sneed WD, Nuckles DB. Shade determination prior to field
isolation. Dent Surv. 1978 Apr;54(3):32.
10. Vanini L,Toffenetti F. Nuovi concetti estetici nell’uso dei ma-
teriali compositi. Quaderni di progresso stomatologico a cura
degli Amici di Brugg. Rimini (Italy); 1995.
About the Author: Dr. Vanini is 11. D’Arcangelo C, Vanini L, Prosperi GD, Di Bussolo G, De Ange-
Professor of Restorative Dentistry, lis F, D’Amario M, Caputi S. The clinical influence of adhesive
University La Sapienza, in Rome, thickness on the microtensile bond strength of three adhesive
Italy; and Visiting Professor of systems. J Adhes Dent. 2009;10(4):1-7.
Restorative Dentistry, University
De La Mediterranee, in Marseilles,
12. Ghivari S, Chandak M, Manvar N. Role of oxygen inhibited
France. Dr. Vanini can be contacted
layer on shear bond strength of composites. J Conserv Dent.
by e-mail at: dott.vanini@libero.it.
2010 Jan;13(1):39-41.
Author Disclosure: Dr. Vanini
develops products and lectures for
Micerium S.p.A. in Avegno, Italy. 13. Peyton JH. Finishing and polishing techniques: direct com-
posite resin restorations. Pract Proced Aesthet Dent. 2004
May;16(4):293-8. jCD
98 Fall 2010 • Volume 26 • Number 3
ne fit:
be it r Be
e m
M red
A ACD Hours C
Ne w 3
CE,
AACD Self-Instruction
Continuing
Education Information
General Information Verification of Participation (VOP)
This continuing education (CE) self-instruction pro- VOP will be sent to AACD members via their My-
gram has been developed by the American Academy AACD account upon pass completion. Log onto
of Cosmetic Dentistry (AACD) and an advisory com- www.aacd.com to sign into your MyAACD account.
mittee of the Journal of Cosmetic Dentistry. For members of the Academy of General Dentistry
(AGD): The AACD will send the AGD proof of your
Eligibility and Cost credits earned on a monthly basis. To do this, AACD
must have your AGD member number on file. Be
The exam is free of charge and is intended for and sure to update your AGD member number in your
available to AACD members only. It is the responsi- AACD member profile on MyAACD.com.
bility of each participant to contact his or her state All participants are responsible for sending proof
board for its requirements regarding acceptance of of earned CE credits to their state dental board or
CE credits. The AACD designates this activity for 3 agency for licensure purposes.
continuing education credits.
Disclaimer
Testing and CE
AACD’s self-instruction exams may not provide
The self-instruction exam comprises 10 multiple- enough comprehensive information for participants
choice questions. To receive course credit, AACD to implement into practice. It is recommended that
members must complete and submit the exam and participants seek additional information as required.
answer at least 70% of the questions correctly. Par- The AACD Self-Instruction Program adheres to the
ticipants will receive tests results immediately after guidelines set forth by the American Dental Asso-
taking the examination online and can only take ciation Continuing Education Recognition Program
each exam once. The exam is scored automatically by (CERP), and the AGD Program Approval for Con-
the AACD’s online testing component. The deadline tinuing Education (PACE).
for completed exams is one calendar year from the
publication date of the issue in which the exam ap- Questions and Feedback
peared. The exam is available online at www.aacd.
com. A current web browser is necessary to complete For questions regarding a specific course, informa-
the exam; no special software is needed. tion regarding your CE credits, or to give feedback on
Note: Although the AACD grants these CE credits, a CE self-instruction exam, please contact the AACD
it is up to the receiving governing body to determine Executive Office by e-mailing meetings@aacd.com
the amount of CE credits they will accept and grant or by calling 800.543.9220 or 608.222.8583.
to participants.
ADA CERP is a service of the American Dental Association to assist dental
professionals in identifying quality providers of continuing dental education.
ADA CERP does not approve or endorse individual courses or instructors, nor
does it imply acceptance of credit hours by boards of dentistry. Concerns or
complaints about a CE provider may be directed to the provider or to ADA
CERP at www.ada.org/goto/cerp.
100 Fall 2010 • Volume 26 • Number 3
CE Test/Vanini
(CE) Exercise No. JCD01
Anterior Composite Restorations (Operative Dentistry) AGD Subject Code: 254
The 10 multiple-choice questions for this Continuing Education (CE) self-instruction exam are based on the article, “Conservative
Composite Restorations that Mimic Nature: A Step-by-Step Anatomical Stratification Technique” by Lorenzo Vanini, DDS, MD.
This article appears on pages 80-98.
The examination is free of charge and available to AACD members only. AACD members must log onto www.aacd.com to take
the exam. Note that only Questions 1 through 5 appear here in the printed version of the Journal; they are for readers’ infor-
mation only. The complete, official self-instruction exam is available online only—completed exams submitted any other way will
not be accepted or processed. A current web browser is necessary to complete the exam; no special software is needed. The AACD
is a recognized credit provider for the Academy of General Dentistry, American Dental Association, and National Association of
Dental Laboratories. For any questions regarding this self-instruction exam, call the AACD at 800.543.9220 or 608.222.9540.
1. Color matching is considered a challenging task in esthetic 4. Which of the following best describes the esthetic
dentistry due to which of the following? problem that occurs when using standard enamel
composite layers?
a. Typical shade guides represent the body and thickness of
natural tooth structures. a. When the material is applied thinly, the value is lowered
and translucency is increased.
b. Dentists have used stratification techniques that are di-
rectly related to the optical properties of the restorative b. Thicker layers of material appear whiter, higher in value,
materials. and lower in translucency.
c. No single explanation for determining tooth color has c. As the thickness of the material increases, the value of
provided an exact solution. the restoration is lowered.
d. The lack of uniformity of the shade guides available with d. When thicker layers are applied evenly, the value is
the restorative materials. raised and the translucency decreases.
2. Value 5. Which of the following is useful when determining
tooth color?
a. is strictly related to enamel.
a. A light source color corrected to 4000K.
b. is lower in the younger biotype.
b. Digital photography.
c. relates to the color intensity of a tooth.
c. Standardized shade guides.
d. is best evaluated using digital color photography.
d. Drying the tooth to show a matte finish.
3. Which of the following is true?
a. Tooth color results from the interaction of dentin To see and take the complete exam, log onto www.aacd.com.
and light.
b. Enamel is responsible for the hue and chroma of a tooth.
c. Fluorescence is created by the tooth’s enamel.
d. Enamel is thicker in mature teeth.
Journal of Cosmetic Dentistry 101
You might also like
- Logic ProblemDocument25 pagesLogic ProblemLaxandra Palomares Chico100% (1)
- Tinting and Toning of Eastman Positive Motion Picture FilmDocument44 pagesTinting and Toning of Eastman Positive Motion Picture FilmSergey Popov0% (1)
- Naturally Aesthetic Restorations and Minimally Invasive DentistryDocument12 pagesNaturally Aesthetic Restorations and Minimally Invasive Dentistrynataly2yoNo ratings yet
- The Stranger in The Photo Is MeDocument4 pagesThe Stranger in The Photo Is MelynnemvtNo ratings yet
- The American Journal of Esthetic DentistryDocument77 pagesThe American Journal of Esthetic DentistryKatiuska HernándezNo ratings yet
- BleachingDocument275 pagesBleachingorthomed100% (4)
- Bio-Emulation Vs UltimoDocument24 pagesBio-Emulation Vs UltimoIlse100% (2)
- Interdisciplinary Treat Planning ChapterDocument56 pagesInterdisciplinary Treat Planning ChapterJulio César Huayllasco de la Cruz0% (1)
- VeneersDocument50 pagesVeneersDr FarhatNo ratings yet
- Digital Smile Design Concept PDFDocument18 pagesDigital Smile Design Concept PDFAndyRamosLopezNo ratings yet
- Smile Design IIDocument68 pagesSmile Design IIkastiel730% (1)
- 10 0000@Www Quintpub Com@ejed@18638Document23 pages10 0000@Www Quintpub Com@ejed@18638Víctor Rodríguez67% (3)
- Smile Analyis and DesignDocument16 pagesSmile Analyis and Designpopat78100% (5)
- Conservative Composite RestorationDocument18 pagesConservative Composite RestorationMoroianu Marius100% (3)
- The "Index Technique" in Worn Dentition - A New and Conservative ApproachDocument32 pagesThe "Index Technique" in Worn Dentition - A New and Conservative ApproachFilipe Queiroz100% (2)
- Endodontics PDFDocument507 pagesEndodontics PDFAndra Andu50% (4)
- Contemporary Esthetic Dentistry, 1E (2012) (PDF) (UnitedVRG) PDFDocument827 pagesContemporary Esthetic Dentistry, 1E (2012) (PDF) (UnitedVRG) PDFAna Rahău100% (8)
- Magne ProvisionalsDocument10 pagesMagne Provisionalsdrdanielsan100% (1)
- Veneer Series PT 1Document6 pagesVeneer Series PT 1Cornelia Gabriela OnuțNo ratings yet
- Journal Esthetic Dentistry 2000Document67 pagesJournal Esthetic Dentistry 2000Jhon Jairo Ojeda Manrique67% (3)
- Minimall Tooth Preparation Garil GurelDocument13 pagesMinimall Tooth Preparation Garil GurelMónica BecerraNo ratings yet
- 2010 02 QDT MAGNE Porcelain Jacket CrownsDocument8 pages2010 02 QDT MAGNE Porcelain Jacket CrownsprosthprosthNo ratings yet
- Smile Analysis Part 2Document11 pagesSmile Analysis Part 2Mircea Ilie100% (1)
- JC Laminates VeneersDocument47 pagesJC Laminates Veneersvarsha palledNo ratings yet
- Smile DesignDocument64 pagesSmile Designbaskarend67% (6)
- Precision in Dental Esthetics PDFDocument463 pagesPrecision in Dental Esthetics PDFTeodor Baciu50% (2)
- Biologically Oriented Preparation Technique (BOPT) : A Ne/a/ Approach For Prosthetic Restoration of Periodontically Healthy TeethDocument15 pagesBiologically Oriented Preparation Technique (BOPT) : A Ne/a/ Approach For Prosthetic Restoration of Periodontically Healthy TeethDr. Marica Ramona Elena100% (1)
- 21 Principles Smile Design Lee OstlerDocument43 pages21 Principles Smile Design Lee OstlerRuxandra Murariu100% (7)
- Protocolo Rehabilitacion OralDocument25 pagesProtocolo Rehabilitacion Oraljotapintor100% (8)
- Adhesive RevolutionDocument8 pagesAdhesive RevolutionErick Lachner100% (5)
- AmericanCinematographer February2022Document79 pagesAmericanCinematographer February2022Fede GiardinaNo ratings yet
- Direct Composite Restorations StratificationDocument18 pagesDirect Composite Restorations Stratificationbubbiexo100% (1)
- Adhesive Restoration of Endodontically Treated TeethFrom EverandAdhesive Restoration of Endodontically Treated TeethRating: 3 out of 5 stars3/5 (2)
- Coachman Pink QDT 2010 PDFDocument15 pagesCoachman Pink QDT 2010 PDFHugoMoralesTecnicoDentalNo ratings yet
- Esthetics Dentistry PDFDocument475 pagesEsthetics Dentistry PDFCHRISTIAN100% (3)
- Porcelain Laminate VeneersDocument66 pagesPorcelain Laminate VeneersneethuNo ratings yet
- The Ideal Restoration of Endodontically Treated Teeth Structural and Esthetic Considerations A Review of The Literature and Clinical Guidelines For The Restorative ClinicianDocument31 pagesThe Ideal Restoration of Endodontically Treated Teeth Structural and Esthetic Considerations A Review of The Literature and Clinical Guidelines For The Restorative ClinicianLuis Alberto Carpio MorenoNo ratings yet
- Rosalind Krauss Photography in The Service of Surrealism, From L'Amour FouDocument24 pagesRosalind Krauss Photography in The Service of Surrealism, From L'Amour Foumeeeemail532280% (5)
- Esthetic Dentistry and Ceramic Restoration, 1edDocument331 pagesEsthetic Dentistry and Ceramic Restoration, 1edMariana RaduNo ratings yet
- Esthetic Inlays & OnlaysDocument32 pagesEsthetic Inlays & OnlaysYousif Abdulla75% (4)
- Smile Design Dental PhotographyDocument3 pagesSmile Design Dental Photographydranilshinde100% (2)
- Smile DesignDocument7 pagesSmile DesignDanilo Macam100% (1)
- Fixed Prosthodontics in Dental PracticeFrom EverandFixed Prosthodontics in Dental PracticeRating: 4 out of 5 stars4/5 (1)
- Silent Invasion by ELLEN CRYSTALLDocument112 pagesSilent Invasion by ELLEN CRYSTALLluniversovibraNo ratings yet
- Tooth WearDocument843 pagesTooth WearRicardo Duarte100% (1)
- SMILE Analysis FormDocument4 pagesSMILE Analysis Formeili1100% (2)
- Light Colour ShadeDocument19 pagesLight Colour ShadeJames Lin100% (1)
- The "Index Technique" in Worn Dentition: A New and Conservative ApproachDocument32 pagesThe "Index Technique" in Worn Dentition: A New and Conservative ApproachHektor Hak100% (1)
- HTTP WWW - Styleitaliano.org Daily Restorative GameDocument10 pagesHTTP WWW - Styleitaliano.org Daily Restorative GameAmee PatelNo ratings yet
- Clinical Detection of Cracked TeethDocument4 pagesClinical Detection of Cracked Teethoceanblue328100% (1)
- Deep Margin ElevationDocument11 pagesDeep Margin Elevationjarodzee100% (4)
- Diastema Closure With Direct Composite Architectural Gingival Contouring.20150306122816Document6 pagesDiastema Closure With Direct Composite Architectural Gingival Contouring.20150306122816Rossye MpfNo ratings yet
- Digital Smile DesignDocument14 pagesDigital Smile DesignSahana RangarajanNo ratings yet
- Int J Esthet Dent 2014 Magne PDFDocument17 pagesInt J Esthet Dent 2014 Magne PDFVanessa Patiño Bautista100% (1)
- Anterior Esthetics - Managing Difficult ChallengesDocument17 pagesAnterior Esthetics - Managing Difficult Challenges881971100% (5)
- Biomimetic AllemanDocument6 pagesBiomimetic AllemanAlireza RaieNo ratings yet
- TMP F643Document20 pagesTMP F643FrontiersNo ratings yet
- Architectural Photography Within The ConDocument14 pagesArchitectural Photography Within The ConmiesNo ratings yet
- Контрольне Оцінювання. i СеместрDocument6 pagesКонтрольне Оцінювання. i Семестрyyyaroslavvv X0% (2)
- Sinar PartsDocument8 pagesSinar PartsBubble FishNo ratings yet
- Camera Mechanics WorkshopDocument52 pagesCamera Mechanics Workshopganesha translatesNo ratings yet
- Edss 450a 7 - Lesson Plan 3 UpdateDocument8 pagesEdss 450a 7 - Lesson Plan 3 Updateapi-605923616No ratings yet
- Chapter 3Document55 pagesChapter 3Chou PotNo ratings yet
- Lubitel 166B: Back To Main On-Line Manual PageDocument10 pagesLubitel 166B: Back To Main On-Line Manual PageWaltNo ratings yet
- Review Metabolism TalksDocument6 pagesReview Metabolism TalksAlina BaldirisNo ratings yet
- Tipos de Colores Pastel Increíbles PDFDocument2 pagesTipos de Colores Pastel Increíbles PDFestephanie andrea francis mejiaNo ratings yet
- PhotojournalismDocument25 pagesPhotojournalismRom Mark Villanueva MacamNo ratings yet
- Reading Pamphlet For PRE-TOEFLDocument74 pagesReading Pamphlet For PRE-TOEFLĐỗ Hải YếnNo ratings yet
- Conceptualism and FeminismDocument8 pagesConceptualism and FeminismOlesia ProkopetsNo ratings yet
- Color Imaging Fundamentals and Applications PDFDocument1,041 pagesColor Imaging Fundamentals and Applications PDFDaniela OliverosNo ratings yet
- 4 Light PrinciplesDocument3 pages4 Light PrinciplesRamesh PatelNo ratings yet
- Without A Trace - Michael FriedDocument11 pagesWithout A Trace - Michael FriedLuis LaroccaNo ratings yet
- Remanufacturing Instructions: Oasis Imaging Products Technical Support (888) 627-6555Document3 pagesRemanufacturing Instructions: Oasis Imaging Products Technical Support (888) 627-6555Hildeu FigueiredoNo ratings yet
- Luke Shopping ListDocument5 pagesLuke Shopping Listapi-687578733No ratings yet
- 12.7 Filling Options: /tikz/fill Image OpacityDocument1 page12.7 Filling Options: /tikz/fill Image OpacityjimusosNo ratings yet
- Final2 RoundDocument14 pagesFinal2 RoundJeth J LungayNo ratings yet
- Heidi Hope Photography: #1 - Not Building AnticipationDocument6 pagesHeidi Hope Photography: #1 - Not Building AnticipationpeterNo ratings yet
- Vaginal Davis's Gospel Truths: Marc SiegelDocument10 pagesVaginal Davis's Gospel Truths: Marc Siegelana garcíaNo ratings yet
- Leia e Interprete o Diálogo A Seguir 9º AnoDocument1 pageLeia e Interprete o Diálogo A Seguir 9º AnoNiviaMariaSilvaSalemeNo ratings yet
- Hikvision Deepinview Anpr Operation: Hikvision Certified Security ProfessionalDocument41 pagesHikvision Deepinview Anpr Operation: Hikvision Certified Security Professionaleduardo urbaNo ratings yet
- Case Study - Instagram Rebranding PDFDocument2 pagesCase Study - Instagram Rebranding PDFAlexa RohnNo ratings yet