You might also like
- Cardiovascular and RespiratoryDocument3 pagesCardiovascular and RespiratoryMilla TanNo ratings yet
- School As A Social SystemDocument15 pagesSchool As A Social SystemHalizah Ramthan88% (8)
- French Revolution Notes - IB Hist ExamDocument12 pagesFrench Revolution Notes - IB Hist ExamAshika I100% (52)
- Performance Based Navigation (PBN)Document40 pagesPerformance Based Navigation (PBN)Bayu Chandra100% (2)
- KSB RPHDocument22 pagesKSB RPHrayggzz_88482611No ratings yet
- Jurnal BTKV Herman 1Document11 pagesJurnal BTKV Herman 1Elyas MuhammadNo ratings yet
- HOOOKUP NEW FOR-WPS OfficeDocument2 pagesHOOOKUP NEW FOR-WPS Officeugochukwuibeaja100% (3)
- An Introduction To The Digital Protection of Power Systems - HarbawiDocument163 pagesAn Introduction To The Digital Protection of Power Systems - HarbawiWalber MoraisNo ratings yet
- Carotid Cavernous Fisstula (CCF)Document78 pagesCarotid Cavernous Fisstula (CCF)Deny Handayanto0% (1)
- Catete RDocument3 pagesCatete ROdalis AltamiranoNo ratings yet
- Massive Right Hemothorax As The Source of Hemorrhagic Shock After Laparoscopic Cholecystectomy - Case Report of A Rare Intraoperative ComplicationDocument3 pagesMassive Right Hemothorax As The Source of Hemorrhagic Shock After Laparoscopic Cholecystectomy - Case Report of A Rare Intraoperative ComplicationDaniel LesmanaNo ratings yet
- Atraumatic BleedingDocument3 pagesAtraumatic BleedingElyas MuhammadNo ratings yet
- Intercostal Drainage Tube or Intracardiac DrainageDocument4 pagesIntercostal Drainage Tube or Intracardiac Drainageamit katejaNo ratings yet
- Subclavianand ProglideDocument7 pagesSubclavianand ProglideRomeo GuevaraNo ratings yet
- Unusual Presentation of Covid-19 in Patient With Acute AbdomenDocument4 pagesUnusual Presentation of Covid-19 in Patient With Acute AbdomenCirugía General HGRNo ratings yet
- Mediastinal Abscess After EndobronchialDocument3 pagesMediastinal Abscess After EndobronchialDm LdNo ratings yet
- Retrograde Insertion of Inferior Vena Cava IVC Filter A Bailout PlanDocument4 pagesRetrograde Insertion of Inferior Vena Cava IVC Filter A Bailout PlanAthenaeum Scientific PublishersNo ratings yet
- s44215 023 00094 7Document5 pagess44215 023 00094 7charlaayasyafefiNo ratings yet
- Respirology Case Reports - 2023 - Bansal - A Customized Multimodality Approach For Prolonged Air Leaks PAL inDocument4 pagesRespirology Case Reports - 2023 - Bansal - A Customized Multimodality Approach For Prolonged Air Leaks PAL infabiolaNo ratings yet
- SeminarioDocument14 pagesSeminarioochoa4aNo ratings yet
- Three Cases of Right Heart Thrombus Using POCUS For The Diagnosis of Thromboembolism in COVID-19Document4 pagesThree Cases of Right Heart Thrombus Using POCUS For The Diagnosis of Thromboembolism in COVID-19Yeimer OrtizNo ratings yet
- Perioperative Management of AdrenalectomyDocument13 pagesPerioperative Management of AdrenalectomyTJ LapuzNo ratings yet
- Rjac 490Document3 pagesRjac 490Bhanu PratapNo ratings yet
- PICC Line TroubleshootingDocument67 pagesPICC Line TroubleshootingTatumNo ratings yet
- Coronary Stent Infections A Case of Pericardial Abscess and Stent Displacement After Repeated PTCA Procedures Which Required An Emergency SurgeryDocument4 pagesCoronary Stent Infections A Case of Pericardial Abscess and Stent Displacement After Repeated PTCA Procedures Which Required An Emergency SurgeryAthenaeum Scientific PublishersNo ratings yet
- Copie de Ma Thèse FinaleDocument6 pagesCopie de Ma Thèse FinaleYannick Aimé BatamackNo ratings yet
- Et0420 MedAffairs MouawadDocument5 pagesEt0420 MedAffairs MouawadAna Silvia LebrOnNo ratings yet
- Parent Vessel Occlusion For Right Cavernous ICA Aneurysm:: XA-CRANIAL VAS INTERVEN (GA&C) of 11.07.2021Document2 pagesParent Vessel Occlusion For Right Cavernous ICA Aneurysm:: XA-CRANIAL VAS INTERVEN (GA&C) of 11.07.2021Sri HarishNo ratings yet
- Case 4Document4 pagesCase 4Hany ElbarougyNo ratings yet
- Clinics in Surgery: Fecopneumothorax Surgery by Thoracoabdominal Incision After Mckeown EsophagectomyDocument2 pagesClinics in Surgery: Fecopneumothorax Surgery by Thoracoabdominal Incision After Mckeown EsophagectomysaraNo ratings yet
- Epidural - Ribs 0000542-200005000-00041Document3 pagesEpidural - Ribs 0000542-200005000-00041Nathania YenatanNo ratings yet
- Apm 12 151 PDFDocument4 pagesApm 12 151 PDFFityan Aulia RahmanNo ratings yet
- Pneumoperitoneum As A Complication of Cardiopulmonary ResuscitationDocument4 pagesPneumoperitoneum As A Complication of Cardiopulmonary Resuscitationl0litaaNo ratings yet
- Case Report: Saudi Journal of Kidney Diseases and TransplantationDocument5 pagesCase Report: Saudi Journal of Kidney Diseases and TransplantationAleksandre KordzadzeNo ratings yet
- Wang A220119JW BLM Formatted 1Document3 pagesWang A220119JW BLM Formatted 1Harold FernandezNo ratings yet
- Fistula BroncobiliarDocument3 pagesFistula Broncobiliarsamuelfdiaz.0103No ratings yet
- Anestesi Low-Dose Spinal Dan Epidural Pada Pasien Syok Hemoragik Yang Akan Dilakukan Histerektomi Dengan Suspek COVID-19Document8 pagesAnestesi Low-Dose Spinal Dan Epidural Pada Pasien Syok Hemoragik Yang Akan Dilakukan Histerektomi Dengan Suspek COVID-19widiastrikNo ratings yet
- The Use of A Vascular Patch CorMatrix ECM® For Reconstruction of Carotid Arteries in The Treatment of Postoperative Wound InfectionDocument3 pagesThe Use of A Vascular Patch CorMatrix ECM® For Reconstruction of Carotid Arteries in The Treatment of Postoperative Wound InfectionMircea Eugen MutuNo ratings yet
- Using VAC To Treat A Vascular Bypass Site Infection: CasereportDocument2 pagesUsing VAC To Treat A Vascular Bypass Site Infection: CasereportamdreyNo ratings yet
- Timetable PosterExDocument45 pagesTimetable PosterExNeo Rodriguez AlvaradoNo ratings yet
- Sub Diaphragmatic Abscess Leading To Empyema Thoracis in A Case of Perforated Appendix A Rare Case ReportDocument4 pagesSub Diaphragmatic Abscess Leading To Empyema Thoracis in A Case of Perforated Appendix A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Resuscitation Complicated by Delayed ObstructiveDocument3 pagesResuscitation Complicated by Delayed ObstructiveFadel AhmadNo ratings yet
- Case Report: Bilateral Pneumothoraces Following Central Venous CannulationDocument4 pagesCase Report: Bilateral Pneumothoraces Following Central Venous Cannulationfernando serrano reyesNo ratings yet
- Severe Pelvic Fracture With Profound Hypotension: A Case Report and Treatment AlgorithmDocument3 pagesSevere Pelvic Fracture With Profound Hypotension: A Case Report and Treatment AlgorithmodyNo ratings yet
- Nasser2015Document5 pagesNasser2015hengkileonardNo ratings yet
- Unilateral Diaphragm Paralysis With COVID-19 InfectionDocument2 pagesUnilateral Diaphragm Paralysis With COVID-19 InfectiontankNo ratings yet
- Unclogging The Effects of The Angiojet Thrombectomy System On Kidney Function: A Case ReportDocument6 pagesUnclogging The Effects of The Angiojet Thrombectomy System On Kidney Function: A Case ReportBruno CoutinhoNo ratings yet
- Dresetal Weaningthecardiacpatient COCC2014Document9 pagesDresetal Weaningthecardiacpatient COCC2014JorgeNo ratings yet
- Pinch Off Syndrome - A Rare Complication of Chemo Port: Dr. C. Ramachandra, Dr. Pavan Kumar J, Dr. C. SrinivasDocument4 pagesPinch Off Syndrome - A Rare Complication of Chemo Port: Dr. C. Ramachandra, Dr. Pavan Kumar J, Dr. C. SrinivasPavan JonnadaNo ratings yet
- Complicated Sinusitis With Sphenopalatine Artery Thrombosis in A COVID-19 Patient, A Case ReportDocument3 pagesComplicated Sinusitis With Sphenopalatine Artery Thrombosis in A COVID-19 Patient, A Case ReportNurul Aisyah PaldarNo ratings yet
- Jurnal VaskularDocument6 pagesJurnal VaskulardrelvNo ratings yet
- Ksap 2015Document98 pagesKsap 2015Nehal ElnagarNo ratings yet
- Unusual Complications of Ultrasound Guided Central Venous CannulationDocument4 pagesUnusual Complications of Ultrasound Guided Central Venous CannulationPrabakaran ParameswaranNo ratings yet
- Emp2 12098Document4 pagesEmp2 12098Miva MaviniNo ratings yet
- Sudden Hypotension Occurring After 4 Days of Left-Sided Central Catheter PlacementDocument3 pagesSudden Hypotension Occurring After 4 Days of Left-Sided Central Catheter PlacementFaqih SultonfaqNo ratings yet
- Case Report Embolic Shotgun Pellet To The Righ 2024 International JournalDocument5 pagesCase Report Embolic Shotgun Pellet To The Righ 2024 International JournalRonald QuezadaNo ratings yet
- Comerota 2010Document5 pagesComerota 2010Jade GomitaNo ratings yet
- 1 s2.0 S2210261223004741 MainDocument5 pages1 s2.0 S2210261223004741 MainDevita SanangkaNo ratings yet
- Isccm PosterDocument3 pagesIsccm PosterPrabakaran ParameswaranNo ratings yet
- Peripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric SurgerDocument8 pagesPeripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric Surgeralergo.ramirezNo ratings yet
- O o o o o o o o o o o oDocument9 pagesO o o o o o o o o o o oAshish PandeyNo ratings yet
- Acute Presentation of Third Ventricular Cavernous Malformation - Saberi2021Document4 pagesAcute Presentation of Third Ventricular Cavernous Malformation - Saberi2021Bruno Diaz LlanesNo ratings yet
- Catheter-Directed Thrombolysis of Iliocaval Thrombosis in Patients With COVID-19Document13 pagesCatheter-Directed Thrombolysis of Iliocaval Thrombosis in Patients With COVID-19oscarNo ratings yet
- Pneumonectomy Management PDFDocument6 pagesPneumonectomy Management PDFMurali BalaNo ratings yet
- Pneumonectomy ManagementDocument6 pagesPneumonectomy ManagementJefferyNo ratings yet
- Annual Update in Intensive Care and Emergency Medicine 2020From EverandAnnual Update in Intensive Care and Emergency Medicine 2020No ratings yet
- MRMCasiCliniciluglio2021 Vol2def1Document69 pagesMRMCasiCliniciluglio2021 Vol2def1stellacharlesNo ratings yet
- Ventilator-Associated Pneumonia Due To Carbapenem-Resistant Providencia RettgeriDocument4 pagesVentilator-Associated Pneumonia Due To Carbapenem-Resistant Providencia RettgeristellacharlesNo ratings yet
- The Cough Re Ex: The Janus of Respiratory Medicine: Frontiers in Physiology June 2021Document9 pagesThe Cough Re Ex: The Janus of Respiratory Medicine: Frontiers in Physiology June 2021stellacharlesNo ratings yet
- Discontinuation Versus Continuation of Renin-AngioDocument11 pagesDiscontinuation Versus Continuation of Renin-AngiostellacharlesNo ratings yet
- Recent Insights Into The Management of Pleural InfDocument15 pagesRecent Insights Into The Management of Pleural InfstellacharlesNo ratings yet
- Recent Insights Into The Measurement of Carbon DioDocument20 pagesRecent Insights Into The Measurement of Carbon DiostellacharlesNo ratings yet
- The Role of Dupilumab in Severe AsthmaDocument15 pagesThe Role of Dupilumab in Severe AsthmastellacharlesNo ratings yet
- Physics Project: Brain Computer InterfaceDocument15 pagesPhysics Project: Brain Computer InterfacestellacharlesNo ratings yet
- Helmet Non-Invasive Ventilation For COVID-19 Patients (Helmet-COVID) : Study Protocol For A Multicentre Randomised Controlled TrialDocument8 pagesHelmet Non-Invasive Ventilation For COVID-19 Patients (Helmet-COVID) : Study Protocol For A Multicentre Randomised Controlled TrialstellacharlesNo ratings yet
- Lesson 8-BridgesDocument2 pagesLesson 8-BridgesMohamed MraouiNo ratings yet
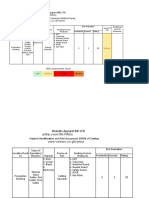
- Brandix Apparel BD LTD: Hazard Identification and Risk Assesment (HIRA) of SwingDocument3 pagesBrandix Apparel BD LTD: Hazard Identification and Risk Assesment (HIRA) of SwingShoaibNo ratings yet
- Mechanisms Final ReportDocument44 pagesMechanisms Final ReportOmar SaleemNo ratings yet
- Technical Data: 1. DescriptionDocument6 pagesTechnical Data: 1. DescriptionRIGOBERTO PONCENo ratings yet
- Logic GatesDocument11 pagesLogic GatesXharmei ThereseNo ratings yet
- Ten Common SQL Server Reporting Services Challenges and SolutionsDocument25 pagesTen Common SQL Server Reporting Services Challenges and Solutionssrisrinivas76No ratings yet
- Nature of ObDocument3 pagesNature of ObLords PorseenaNo ratings yet
- Altivar Process ATV900 - VW3A7747Document5 pagesAltivar Process ATV900 - VW3A7747Adrian Pacori ParedesNo ratings yet
- 9 Gitterstar LoadTable Autom TrucksDocument1 page9 Gitterstar LoadTable Autom TrucksSnaz_nedainNo ratings yet
- Opnav 4855 1aDocument8 pagesOpnav 4855 1aRobert ValeNo ratings yet
- Sexual HarassmentDocument11 pagesSexual HarassmentKrip KNo ratings yet
- ATS - DC Couple - System Principle Diagram20191115Document1 pageATS - DC Couple - System Principle Diagram20191115Syed Furqan RafiqueNo ratings yet
- Properties of Laplace Transform - ROCDocument5 pagesProperties of Laplace Transform - ROCrachit guptaNo ratings yet
- ASSESSMENT IN LEARNING 2 MODULE (Finals) With POSTTESTDocument63 pagesASSESSMENT IN LEARNING 2 MODULE (Finals) With POSTTESTcreqyaqaNo ratings yet
- Packaged CCE Software Compatibility Matrix For 11.5 (X)Document14 pagesPackaged CCE Software Compatibility Matrix For 11.5 (X)eduardo perezNo ratings yet
- Chest Tubes Nursing CareDocument2 pagesChest Tubes Nursing CareYousef KhalifaNo ratings yet
- RedBOOK On Dimensional Modelling IBMDocument668 pagesRedBOOK On Dimensional Modelling IBMapi-3701383100% (3)
- Module 1 Chapter 3 Week 3 Fundamentals of Surveying LectureDocument12 pagesModule 1 Chapter 3 Week 3 Fundamentals of Surveying LecturePrincess Erika CanlasNo ratings yet
- Siemens Dr. Surachai Presentation Energy4.0Document24 pagesSiemens Dr. Surachai Presentation Energy4.0Sittiporn KulsapsakNo ratings yet
- Energy Balance: Technological Institute of The PhilippinesDocument56 pagesEnergy Balance: Technological Institute of The Philippineshenriel tambioNo ratings yet
- Injection Pres Op GasDocument2 pagesInjection Pres Op GasSrWilson Z AriasNo ratings yet
- 8th Sem - Assignment - MD II (2962108)Document5 pages8th Sem - Assignment - MD II (2962108)rishabhk28995No ratings yet
- Danielle Cuomo Updated ResumeDocument1 pageDanielle Cuomo Updated Resumeapi-261843379No ratings yet
- CostcoDocument96 pagesCostcoChris DavidsonNo ratings yet