You might also like
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Clin Management Post Op Pain Web AlgorithmDocument22 pagesClin Management Post Op Pain Web AlgorithmwanggaNo ratings yet
- Clin Management Cancer Pain Pedi Web AlgorithmDocument28 pagesClin Management Cancer Pain Pedi Web AlgorithmRuben Santiago LassoNo ratings yet
- Anaesthesia - 2021 - Feray - PROSPECT Guidelines For Video Assisted Thoracoscopic Surgery A Systematic Review andDocument15 pagesAnaesthesia - 2021 - Feray - PROSPECT Guidelines For Video Assisted Thoracoscopic Surgery A Systematic Review andboby abdul rahmanNo ratings yet
- Epidural Infusion Heart of England TrustDocument19 pagesEpidural Infusion Heart of England TrustkhalidNo ratings yet
- Pain Management After Open Liver Resection: Procedure-Specific Postoperative Pain Management (PROSPECT) RecommendationsDocument13 pagesPain Management After Open Liver Resection: Procedure-Specific Postoperative Pain Management (PROSPECT) RecommendationsdrsubramanianNo ratings yet
- Laminectomy: Notes On PROSPECT RecommendationsDocument5 pagesLaminectomy: Notes On PROSPECT RecommendationsWidya AriatyNo ratings yet
- Postoperative Pain Literature ReviewDocument7 pagesPostoperative Pain Literature Reviewafduaciuf100% (1)
- Analgesic Effects and Adverse Reactions of LidocaiDocument6 pagesAnalgesic Effects and Adverse Reactions of Lidocaibrendastevany23No ratings yet
- E044168 FullDocument7 pagesE044168 FulldrmelinjoeNo ratings yet
- Acute Pain Management Clinics 2014Document10 pagesAcute Pain Management Clinics 2014Veronica Romero MouthonNo ratings yet
- Lra 181458 Non Operating Room Anesthesia Patient Selection and SpecialDocument9 pagesLra 181458 Non Operating Room Anesthesia Patient Selection and SpecialEric Aguilar SantiagoNo ratings yet
- 3. Bài Báo Tiếng Anh Khác Tên Tác GiảDocument5 pages3. Bài Báo Tiếng Anh Khác Tên Tác GiảnamanesthesiaNo ratings yet
- Cigna 2017Document20 pagesCigna 2017Bishara WilsonNo ratings yet
- Effectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialDocument13 pagesEffectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialgigicarvajalNo ratings yet
- Pogatzki Zahn2017Document16 pagesPogatzki Zahn2017Indra IhsanNo ratings yet
- Student medication interactionsDocument26 pagesStudent medication interactionsLila DanielsNo ratings yet
- Advances in The Management of Persistent Pain.110Document5 pagesAdvances in The Management of Persistent Pain.110EmaDiaconuNo ratings yet
- Jurnal LaparatomyDocument12 pagesJurnal LaparatomyindahmartyasNo ratings yet
- New Epidural ProtocolDocument16 pagesNew Epidural ProtocolAndreea OanaNo ratings yet
- Management of Acute Pain and Chronic Noncancer Pain: Section IVDocument12 pagesManagement of Acute Pain and Chronic Noncancer Pain: Section IVRizky DimasaputraNo ratings yet
- Terapia Del Dolor CancerDocument11 pagesTerapia Del Dolor CancerJean Brando Torres GuerreroNo ratings yet
- SassercDocument25 pagesSassercapi-708014280No ratings yet
- Multimodal Pain Management: PropertiesDocument5 pagesMultimodal Pain Management: PropertiesTanushree PanjariNo ratings yet
- Royal College X AnesthesiaDocument66 pagesRoyal College X AnesthesiaManuela CormioNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Assessment and Management of Delirium in Pediatric PatientsDocument7 pagesAssessment and Management of Delirium in Pediatric PatientsEunike Karamoy100% (1)
- Journal Reading AnestesiDocument4 pagesJournal Reading AnestesiVania RNo ratings yet
- Multimodal Postoperative Analgesia: Combinations of Analgesics After Abdominal Surgery at Chu - Jra AntananarivoDocument11 pagesMultimodal Postoperative Analgesia: Combinations of Analgesics After Abdominal Surgery at Chu - Jra AntananarivoIJAR JOURNALNo ratings yet
- Orthopaedic Knee Referral GuidelinesDocument7 pagesOrthopaedic Knee Referral GuidelinesMilka DatuNo ratings yet
- Otc Advisor PainDocument24 pagesOtc Advisor Painfarzad100% (2)
- 1.04 (Surgery) Anesthesiology Part 1Document5 pages1.04 (Surgery) Anesthesiology Part 1Leo Mari Go LimNo ratings yet
- (Anes) 1 - Preanesthetic Evaluation (Dra. Luna-Gomez) ?Document5 pages(Anes) 1 - Preanesthetic Evaluation (Dra. Luna-Gomez) ?NoreenNo ratings yet
- Final Sup Bree AMDGPostop Pain 091318 WcoverDocument14 pagesFinal Sup Bree AMDGPostop Pain 091318 WcoveroNo ratings yet
- University of Cebu-Lapulapu and Mandaue A.C Cortes Avenue, Looc, Mandaue City College of NursingDocument10 pagesUniversity of Cebu-Lapulapu and Mandaue A.C Cortes Avenue, Looc, Mandaue City College of NursingSean Menard FloresNo ratings yet
- Literature Review On Postoperative Pain ManagementDocument6 pagesLiterature Review On Postoperative Pain Managementea4c954qNo ratings yet
- 1 s2.0 S2468824X17300517 MainDocument5 pages1 s2.0 S2468824X17300517 MainFirah Triple'sNo ratings yet
- CCT in Anaesthetics Core Level TrainingDocument99 pagesCCT in Anaesthetics Core Level TrainingparuNo ratings yet
- Analgesia Multimodal en Cirugía AmbulatoriaDocument7 pagesAnalgesia Multimodal en Cirugía AmbulatoriaChurrunchaNo ratings yet
- Pain Priorities in Pre-Hospital CareDocument3 pagesPain Priorities in Pre-Hospital CareANNIX FERRERNo ratings yet
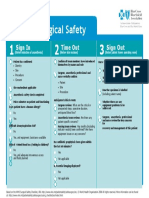
- Surgical Safety: Sign in Time Out Sign OutDocument1 pageSurgical Safety: Sign in Time Out Sign OutNathanNo ratings yet
- 1 s2.0 S1521689614000044 PDFDocument21 pages1 s2.0 S1521689614000044 PDFAida TantriNo ratings yet
- Hyponatremia Inpatient Management of JCG0342 V3Document12 pagesHyponatremia Inpatient Management of JCG0342 V3zikryauliaNo ratings yet
- Simulated Care (Bajado)Document6 pagesSimulated Care (Bajado)Ma. Ferimi Gleam BajadoNo ratings yet
- Anesthesia For Orthopedic Trauma - UpToDateDocument36 pagesAnesthesia For Orthopedic Trauma - UpToDatematheusbbragacNo ratings yet
- Journal Homepage: - : IntroductionDocument4 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- AA 53279 An Overview of Anesthetic Procedures Tools and Techniques I 012715Document8 pagesAA 53279 An Overview of Anesthetic Procedures Tools and Techniques I 012715Aulia Muzizatun FitrianiNo ratings yet
- PregabalinaDocument5 pagesPregabalinaema moralesNo ratings yet
- Evaluating The Implementation of A Preemptive,.5Document7 pagesEvaluating The Implementation of A Preemptive,.5โสภาพรรณวดี รวีวารNo ratings yet
- Epidural Intraspinal Anticoagulation Guidelines - UKDocument9 pagesEpidural Intraspinal Anticoagulation Guidelines - UKjoshNo ratings yet
- Anaesthesia - 2008 - Fischer - A Procedure Specific Systematic Review and Consensus Recommendations For PostoperativeDocument19 pagesAnaesthesia - 2008 - Fischer - A Procedure Specific Systematic Review and Consensus Recommendations For PostoperativemclimacoNo ratings yet
- Sickle Cell Disease ED Vasocclusive Crises Pain Management GuidelineDocument1 pageSickle Cell Disease ED Vasocclusive Crises Pain Management GuidelineLakshmanan KrishnamurtiNo ratings yet
- Emergency Department Guideline: Laceration RepairDocument4 pagesEmergency Department Guideline: Laceration RepairSalman AssiriNo ratings yet
- Coba 2Document6 pagesCoba 2Bianca CaterinalisendraNo ratings yet
- Analgesic Efficacy of Erector Spinae Plane BlocksDocument7 pagesAnalgesic Efficacy of Erector Spinae Plane BlocksAlejandra SanchezNo ratings yet
- Complete - Nursing Care Plan - Group4Document10 pagesComplete - Nursing Care Plan - Group4TaanzNo ratings yet
- Orbital Trauma NCP and Drug StudyDocument5 pagesOrbital Trauma NCP and Drug StudyDersly LaneNo ratings yet
- Beri151216 w1Document1 pageBeri151216 w1Lunatiku TraderNo ratings yet
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamNo ratings yet
- AnesthesiaDocument44 pagesAnesthesiamaher ahmadNo ratings yet
- System Patient Care ServicesDocument15 pagesSystem Patient Care Servicesscan resepNo ratings yet
- Handbook of Pain ManagementDocument730 pagesHandbook of Pain Managementanon_990504998100% (6)
- Pain Management in Nursing Practice of Intensive Care Postoperational Stage PatientsDocument9 pagesPain Management in Nursing Practice of Intensive Care Postoperational Stage PatientsFhietry Idrus ScaftweeNo ratings yet
- Dolor Crònic AlbertaDocument27 pagesDolor Crònic AlbertaJosep Gonzalez - CrydaNo ratings yet
- Postoperative Pain ControlDocument18 pagesPostoperative Pain ControlRafael Eduardo Toro ManotasNo ratings yet
- Pain Management in Palliative CareDocument45 pagesPain Management in Palliative CarePGDME 20192020No ratings yet
- Eusem Epi Guidelines March 2020 PDFDocument92 pagesEusem Epi Guidelines March 2020 PDFАлекс КейNo ratings yet
- Assessment and Management of Pain: Third EditionDocument104 pagesAssessment and Management of Pain: Third EditionJefry ArieNo ratings yet
- Manajemen NyeriDocument2 pagesManajemen Nyeriscan resepNo ratings yet
- Vital Sign PainDocument50 pagesVital Sign Painscan resepNo ratings yet
- Guidelines At-A-Glance-ADocument4 pagesGuidelines At-A-Glance-Aapi-395709033No ratings yet
- Postoperative Pain Management - ESRA GuidelinesDocument34 pagesPostoperative Pain Management - ESRA GuidelinesAlex Apsokardos100% (1)
- Obat NyeriDocument51 pagesObat Nyeriscan resepNo ratings yet
- Joint Statement On Pain ManagementDocument5 pagesJoint Statement On Pain Managementscan resepNo ratings yet
- Tenneses PainDocument4 pagesTenneses Painscan resepNo ratings yet
- Pain NHSDocument54 pagesPain NHSscan resepNo ratings yet
- Pain Care ManagementDocument108 pagesPain Care Managementscan resepNo ratings yet
- Pain: Current Understanding of Assessment, Management, and TreatmentsDocument101 pagesPain: Current Understanding of Assessment, Management, and TreatmentsNational Pharmaceutical Council100% (8)
- Protokol NyeriDocument5 pagesProtokol Nyeriscan resepNo ratings yet
- AAFP NyeriDocument40 pagesAAFP Nyeriscan resepNo ratings yet
- HOSPITAL STRATEGIES FOR PAIN AND OPIOID USEDocument4 pagesHOSPITAL STRATEGIES FOR PAIN AND OPIOID USEscan resepNo ratings yet
- Sign 136Document71 pagesSign 136Mariana Martinez LechugaNo ratings yet
- Manajemen Nyeri Dengan OpioidDocument4 pagesManajemen Nyeri Dengan Opioidscan resepNo ratings yet
- Eipt 017 001 PDFDocument31 pagesEipt 017 001 PDFWija OgieNo ratings yet
- Managing PainDocument44 pagesManaging Painscan resepNo ratings yet
- 1 - Pain - Management - LR PDFDocument96 pages1 - Pain - Management - LR PDFAgusBhaktiNo ratings yet
- Practice Guidelines For Chronic Pain Management PDFDocument24 pagesPractice Guidelines For Chronic Pain Management PDFAlexandraTomoiuNo ratings yet
- Pain Management Guidelines - HCANJ May 12 Final PDFDocument30 pagesPain Management Guidelines - HCANJ May 12 Final PDFPratama PuteraNo ratings yet
- 1 - Pain - Management - LR PDFDocument96 pages1 - Pain - Management - LR PDFAgusBhaktiNo ratings yet
- OrganTrade ProefschriftFrederikeAmbagtsheer PDFDocument225 pagesOrganTrade ProefschriftFrederikeAmbagtsheer PDFJanani SankarNo ratings yet
- Improvement of Pregnant Women Visit in Puskesmas As An Effect of Using Ultrasound in Pregnancy ExaminationDocument12 pagesImprovement of Pregnant Women Visit in Puskesmas As An Effect of Using Ultrasound in Pregnancy ExaminationKharinaNo ratings yet
- MERGEFDocument383 pagesMERGEFmadison DeliNo ratings yet
- DulcolaxDocument1 pageDulcolaxKatie McPeekNo ratings yet
- Lip AugmentationDocument8 pagesLip AugmentationAhmed BadawyNo ratings yet
- Open LetterDocument3 pagesOpen Letterapi-652435946No ratings yet
- Otc Template Pi PholcodineDocument3 pagesOtc Template Pi PholcodineLucinda RuckleyNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument8 pagesNew Microsoft Office PowerPoint Presentationjenny girlNo ratings yet
- Executive Rule For CME - PD - SCFHSDocument14 pagesExecutive Rule For CME - PD - SCFHSsevattapillaiNo ratings yet
- Perbandingan Percepatan Penyembuhan Luka Sirkumsisi Menggunakan Elektrocauter Dengan Modern Klem Di Wilayah Kerja Puskesmas Pembantu LiangDocument5 pagesPerbandingan Percepatan Penyembuhan Luka Sirkumsisi Menggunakan Elektrocauter Dengan Modern Klem Di Wilayah Kerja Puskesmas Pembantu LiangEman SulaemanNo ratings yet
- QuizDocument2 pagesQuizTimmy CarasNo ratings yet
- A Polymerase Chain Reaction-Based Algorithm To Detect and Prevent Transmission of Adenoviral Conjunctivitis in Hospital EmployeesDocument10 pagesA Polymerase Chain Reaction-Based Algorithm To Detect and Prevent Transmission of Adenoviral Conjunctivitis in Hospital EmployeesWiyaah AsNo ratings yet
- Monitoring Vital Signs Detects COVID-19 Using WearablesDocument7 pagesMonitoring Vital Signs Detects COVID-19 Using WearablesMaxandrea Beatrice ArmillaNo ratings yet
- UntitledDocument41 pagesUntitledgladyannNo ratings yet
- Posterior Retroperitoneoscopic AdrenalectomyDocument14 pagesPosterior Retroperitoneoscopic AdrenalectomyShreyNo ratings yet
- Diams PDFDocument80 pagesDiams PDFDr.Mohammed Mustafa Iqbal100% (3)
- Nrs 2002 Form PDF - Google SearchDocument1 pageNrs 2002 Form PDF - Google SearchsandeepNo ratings yet
- Still, Founder of OsteopathyDocument236 pagesStill, Founder of OsteopathyJAVIER GARCIANo ratings yet
- Unidad 2. Tarea 2. EscrituraDocument5 pagesUnidad 2. Tarea 2. EscrituraAndrea ChavarroNo ratings yet
- Rosicrucian 009317Document16 pagesRosicrucian 009317nicolasaraujo100% (1)
- Respiratory FailureDocument15 pagesRespiratory FailureJulien TorresNo ratings yet
- AIIMS Protocol On Shock 2019Document16 pagesAIIMS Protocol On Shock 2019gaddam narasimhaNo ratings yet
- Scrub Nurse Mastectomy DutiesDocument6 pagesScrub Nurse Mastectomy DutiesJeroham R. CoNo ratings yet
- Professional RNDocument2 pagesProfessional RNapi-121454402No ratings yet
- ACOG Abnormal Uterine Bleeding DiagnosisDocument11 pagesACOG Abnormal Uterine Bleeding DiagnosisJimmy Crack CornsNo ratings yet
- Manual urinalysis guideDocument37 pagesManual urinalysis guideAdhya TiaraNo ratings yet
- Tata Memorial Centre Final Add V 020513Document6 pagesTata Memorial Centre Final Add V 020513Rupal SojitraNo ratings yet
- Fever and HyperthermiaDocument9 pagesFever and HyperthermiaMarwan M.100% (1)
- 2 Transcripts From The New Science of Ancient MedicinesDocument24 pages2 Transcripts From The New Science of Ancient MedicinesJorge Garcia SilesNo ratings yet
- Journal Review2Document7 pagesJournal Review2api-589685298No ratings yet
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Summary: Psycho-Cybernetics: by Maxwell Maltz: Key Takeaways, Summary & AnalysisFrom EverandSummary: Psycho-Cybernetics: by Maxwell Maltz: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (2)
- Are You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersFrom EverandAre You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersRating: 5 out of 5 stars5/5 (28)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1243)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)