You might also like
- Family Systems Therapy and AddictionDocument30 pagesFamily Systems Therapy and AddictionthegavmanNo ratings yet
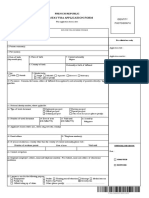
- Form Visa ÝDocument3 pagesForm Visa ÝHo ThanhtuyenNo ratings yet
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- Sylvia Lavin - Architecture in Extremis PDFDocument12 pagesSylvia Lavin - Architecture in Extremis PDFXiaoying Ma100% (1)
- Health Declaration Form DOT AmendedDocument1 pageHealth Declaration Form DOT AmendedImee S. YuNo ratings yet
- Health Declaration Form: or Giving False Information Is Punishable in Accordance With Philippine LawsDocument1 pageHealth Declaration Form: or Giving False Information Is Punishable in Accordance With Philippine LawsJamel AgantalNo ratings yet
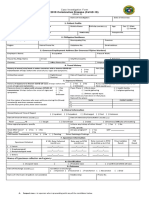
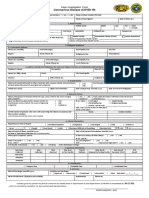
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument4 pagesCoronavirus Disease (COVID-19) : Case Investigation FormMaria JoselaNo ratings yet
- Chapter 6 (Cell Kinetics and Fermenter Design-127-175) PDFDocument49 pagesChapter 6 (Cell Kinetics and Fermenter Design-127-175) PDFOnyx Xyno100% (2)
- Siemens Acuson Sc2000 General Cardiologist Flyer v2Document4 pagesSiemens Acuson Sc2000 General Cardiologist Flyer v2bashir019No ratings yet
- New Cif FormDocument2 pagesNew Cif FormNovie FeneciosNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- CoViD19-Covid Investigation FormDocument1 pageCoViD19-Covid Investigation FormMc Arem PaghunasanNo ratings yet
- CoViD19-CIF-v6-Fillable QCv3-2Document1 pageCoViD19-CIF-v6-Fillable QCv3-2Patrice De CastroNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormChamee MallillinNo ratings yet
- CIF TemplateDocument2 pagesCIF Templateluvaire23No ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- Case Lnvestigation FormDocument3 pagesCase Lnvestigation FormChum ChitaruNo ratings yet
- 2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileDocument1 page2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileMarythel CamachoNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- DOH PIDSR COVID-19 CIF TemplateDocument1 pageDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNo ratings yet
- Revised SSQ&AFDocument16 pagesRevised SSQ&AFSushant NathNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- DOT Health Declaration FormDocument1 pageDOT Health Declaration Formmark nielsen limNo ratings yet
- CIF (For BMDL PhilHealth Purposes Only)Document1 pageCIF (For BMDL PhilHealth Purposes Only)BALIUAG DISTRICT LABORATORYNo ratings yet
- Health Declaration Form of Dot Adopted by The Aquino Center For EventsDocument1 pageHealth Declaration Form of Dot Adopted by The Aquino Center For EventsLui SantosNo ratings yet
- Saric CifDocument1 pageSaric CifMarav SymbNo ratings yet
- DOT Health Declaration FormDocument1 pageDOT Health Declaration FormLouie Silvestre BasaNo ratings yet
- Application For Visa or Transit VisaDocument3 pagesApplication For Visa or Transit VisamagretNo ratings yet
- Form 1-Scc: (Ang Bawat Panig Ay Ang Mga Sumusunod)Document9 pagesForm 1-Scc: (Ang Bawat Panig Ay Ang Mga Sumusunod)Sandy CelineNo ratings yet
- B.L.I.S.T.T Health Declaration Form: Baguio - La Trinidad - Itogon - Sablan - Tuba - TublayDocument1 pageB.L.I.S.T.T Health Declaration Form: Baguio - La Trinidad - Itogon - Sablan - Tuba - TublayLC LeeNo ratings yet
- Philippine Integrated Disease Surveillance and Response: 14 DaysDocument1 pagePhilippine Integrated Disease Surveillance and Response: 14 DaysAlpha BatteryNo ratings yet
- China Visa QuestionnaireDocument5 pagesChina Visa Questionnairepmd20190707No ratings yet
- BCMDDC Covid-19 Health ChecklistsDocument2 pagesBCMDDC Covid-19 Health ChecklistsArvin Talatayod CanteroNo ratings yet
- Self Declaration Form - 0Document1 pageSelf Declaration Form - 0idea pdrlNo ratings yet
- F001 OP R Encoding SheetDocument2 pagesF001 OP R Encoding SheetAnnalien AlaanNo ratings yet
- IST Faculty Application Form 22 May 2023Document5 pagesIST Faculty Application Form 22 May 2023Noman AsgharNo ratings yet
- CT-FORM-BLANKDocument3 pagesCT-FORM-BLANKArce RostumNo ratings yet
- Released: Sunpower Philippines Medical Screening Form (MSF)Document2 pagesReleased: Sunpower Philippines Medical Screening Form (MSF)glenn dalesNo ratings yet
- Job Application FormDocument3 pagesJob Application FormNur FarahinNo ratings yet
- Long-Stay Visa Application Form: French RepublicDocument3 pagesLong-Stay Visa Application Form: French RepublicFaye Isabelle SantiagoNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormcharleneNo ratings yet
- Manship App FormDocument4 pagesManship App Formjonheric2009No ratings yet
- B.L.I.S.T.T Health Declaration Form: Baguio - La Trinidad - Itogon - Sablan - Tuba - TublayDocument1 pageB.L.I.S.T.T Health Declaration Form: Baguio - La Trinidad - Itogon - Sablan - Tuba - TublayLC LeeNo ratings yet
- Guest Registration and Health Declaration FormDocument2 pagesGuest Registration and Health Declaration FormRech YcelNo ratings yet
- Guest Registration and Health Declaration Form 1Document2 pagesGuest Registration and Health Declaration Form 1Rhyx Houell AmboteNo ratings yet
- Visas Hoshi Kim I HonDocument5 pagesVisas Hoshi Kim I Honmacristina546No ratings yet
- Latest HEALTH DECLARATION FORM PDFDocument1 pageLatest HEALTH DECLARATION FORM PDFattydebbiedulay8876No ratings yet
- Request For Orders To Stop Harassment (Civil Harassment)Document4 pagesRequest For Orders To Stop Harassment (Civil Harassment)kakuNo ratings yet
- Soccer Registration FormDocument2 pagesSoccer Registration FormmikevalhallNo ratings yet
- Visitors Health Check List: TemperatureDocument1 pageVisitors Health Check List: TemperatureSterben ShouchiNo ratings yet
- Lloyds Registration Form V3 Jordan Fraser'Document5 pagesLloyds Registration Form V3 Jordan Fraser'my odfNo ratings yet
- CT Form BlankDocument3 pagesCT Form BlankArce RostumNo ratings yet
- Uolus Kandidatų Anketa ENDocument3 pagesUolus Kandidatų Anketa ENABID AKHTERNo ratings yet
- The Major and The Judge: The Inside Story of the War Against COVIDFrom EverandThe Major and The Judge: The Inside Story of the War Against COVIDNo ratings yet
- Tlo7 Kinetics of A Particle Work and EnergyDocument9 pagesTlo7 Kinetics of A Particle Work and EnergyOnyx XynoNo ratings yet
- Untitled DocumentDocument4 pagesUntitled DocumentOnyx XynoNo ratings yet
- S Announcement 20451Document47 pagesS Announcement 20451Onyx XynoNo ratings yet
- Problem Set QuantiDocument1 pageProblem Set QuantiOnyx XynoNo ratings yet
- Cped: Take-Home Activity: General InstructionsDocument1 pageCped: Take-Home Activity: General InstructionsOnyx XynoNo ratings yet
- Hazardous-Waste Part 1Document3 pagesHazardous-Waste Part 1Onyx XynoNo ratings yet
- Dizi Bamboo Flute Chart PDFDocument1 pageDizi Bamboo Flute Chart PDFOnyx XynoNo ratings yet
- S Announcement 25288 PDFDocument5 pagesS Announcement 25288 PDFOnyx XynoNo ratings yet
- S Announcement 25288 PDFDocument5 pagesS Announcement 25288 PDFOnyx XynoNo ratings yet
- 4.code of Ethics For Chemical EngineersDocument103 pages4.code of Ethics For Chemical EngineersOnyx Xyno100% (1)
- Iwaste Hardness PDFDocument5 pagesIwaste Hardness PDFOnyx XynoNo ratings yet
- 4.code of Ethics For Chemical EngineersDocument103 pages4.code of Ethics For Chemical EngineersOnyx Xyno100% (1)
- Catalysts: Porosity Design of Shaped Zeolites For Improved Catalyst Lifetime in The Methanol-to-Hydrocarbons ReactionDocument11 pagesCatalysts: Porosity Design of Shaped Zeolites For Improved Catalyst Lifetime in The Methanol-to-Hydrocarbons ReactionOnyx XynoNo ratings yet
- Colak Foamed GypsumDocument8 pagesColak Foamed GypsumOnyx XynoNo ratings yet
- Placenta Previa Journal KristalDocument23 pagesPlacenta Previa Journal KristalGabbyNo ratings yet
- Tatalaksana Dan Prognosis Severe Visual Impairment Pada Miopia Patologi - Nikho Melga ShalimDocument14 pagesTatalaksana Dan Prognosis Severe Visual Impairment Pada Miopia Patologi - Nikho Melga ShalimOt PtkNo ratings yet
- Health Lesson 1 Dangers of Cigarette SmokingDocument103 pagesHealth Lesson 1 Dangers of Cigarette SmokingKathleen Gail RagaNo ratings yet
- Er Ap Y.O RG: Pulsed Shortwave Therapy (PSWD / PSWT)Document6 pagesEr Ap Y.O RG: Pulsed Shortwave Therapy (PSWD / PSWT)Walter PelaezNo ratings yet
- National Health MissionDocument31 pagesNational Health MissionAlpana Rani DasNo ratings yet
- Jurnal: Andi Nur Mutmainnah Pembimbing: Dr. Adnan Ibrahim, SP - PDDocument7 pagesJurnal: Andi Nur Mutmainnah Pembimbing: Dr. Adnan Ibrahim, SP - PDNur MutmainnahNo ratings yet
- Benefits and Contributions Schedule 2021Document72 pagesBenefits and Contributions Schedule 2021MarcoNo ratings yet
- Group 3-DIALYSISDocument62 pagesGroup 3-DIALYSISFesto HakiNo ratings yet
- Strauman BLX Product Catalog - 450.012-A-En - LowDocument22 pagesStrauman BLX Product Catalog - 450.012-A-En - LowDiyaa SakrNo ratings yet
- Planning Physical Facilities of Hospital and Educational InstitutionDocument5 pagesPlanning Physical Facilities of Hospital and Educational InstitutionSundaraBharathi100% (2)
- Leukocytes or White Blood Cells (WBC)Document22 pagesLeukocytes or White Blood Cells (WBC)Md Atikur AminNo ratings yet
- Read Online Textbook Behavior Modification What It Is and How To Do It 10Th Edition Garry Martin Ebook All Chapter PDFDocument22 pagesRead Online Textbook Behavior Modification What It Is and How To Do It 10Th Edition Garry Martin Ebook All Chapter PDFhilda.rufe918100% (2)
- Nursing Care Plan: Wong's Nursing Care of Infants and Children, 8 Ed. Pg. 324Document3 pagesNursing Care Plan: Wong's Nursing Care of Infants and Children, 8 Ed. Pg. 324Erle Gray CadangenNo ratings yet
- SofPort AOV Patient LeafletDocument8 pagesSofPort AOV Patient LeafletGp MishraNo ratings yet
- Removable Prosthodontics: Louis Blatterfein S. Howard PayneDocument6 pagesRemovable Prosthodontics: Louis Blatterfein S. Howard PayneArjun NarangNo ratings yet
- Vasculitis: Ameen Kabaha, MD Wolfson Medical CenterDocument68 pagesVasculitis: Ameen Kabaha, MD Wolfson Medical Centeranaskabaha100% (1)
- Neuro AssDocument33 pagesNeuro AssImee Balbido MallariNo ratings yet
- Profil PhenobarbitalDocument2 pagesProfil PhenobarbitalOana Maria AndreiNo ratings yet
- Archery Parental ConsentDocument1 pageArchery Parental ConsentleightertonprimaryNo ratings yet
- Information For Patients Needing Irradiated BloodDocument8 pagesInformation For Patients Needing Irradiated BloodCaddy MkaNo ratings yet
- Post-Induction Hypotension and Intraoperative Hypotension As Potential Separate Risk Factors For The Adverse Outcome A Cohort StudyDocument9 pagesPost-Induction Hypotension and Intraoperative Hypotension As Potential Separate Risk Factors For The Adverse Outcome A Cohort Studyfranco vidalNo ratings yet
- 13-Neuroprognostication Algorithm 2021Document1 page13-Neuroprognostication Algorithm 2021khaledNo ratings yet
- DMD Oral-Surgery-430-440Document77 pagesDMD Oral-Surgery-430-440gNo ratings yet
- Ototoxic BrochureDocument6 pagesOtotoxic BrochureWindaNo ratings yet
- NCP 2023Document3 pagesNCP 2023Jannina Barella (SHS)No ratings yet
- ICDAS Dental CariesDocument6 pagesICDAS Dental CariestulusNo ratings yet
- MSN 571 Mid-Term Pharmacology QuestionsDocument13 pagesMSN 571 Mid-Term Pharmacology QuestionsNelson MandelaNo ratings yet