You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Company Industry Employee Count Country: Plastic OmniumDocument4 pagesCompany Industry Employee Count Country: Plastic OmniumA AlamNo ratings yet
- Polycythemi A: Presented By: Palaran, Nina Mae CDocument16 pagesPolycythemi A: Presented By: Palaran, Nina Mae CJichutreasureNo ratings yet
- English - JapanDocument2 pagesEnglish - JapanJoseNo ratings yet
- Agency ArchiveDocument413 pagesAgency ArchiveAZ 211100% (3)
- Cognitive Behaviour Therapy (CBT)Document117 pagesCognitive Behaviour Therapy (CBT)Roslan Ahmad FuadNo ratings yet
- CVA DVA Werkstuk Bekele - tcm39 91310Document40 pagesCVA DVA Werkstuk Bekele - tcm39 91310s_75No ratings yet
- Case Study AmulDocument6 pagesCase Study AmulTales Of TanviNo ratings yet
- Medinaresume 18Document2 pagesMedinaresume 18api-400080530No ratings yet
- Test Bank For Clinical Assessment in Respiratory Care 6th Edition WilkinsDocument19 pagesTest Bank For Clinical Assessment in Respiratory Care 6th Edition Wilkinsfideliamaximilian7pjjf100% (22)
- Reaction To EJKDocument9 pagesReaction To EJKKevin DawangNo ratings yet
- Faculty 460 Eng 334 Kust20201 l2 p2 Paragraph WritingDocument20 pagesFaculty 460 Eng 334 Kust20201 l2 p2 Paragraph WritingMuhammad UsmanNo ratings yet
- Direct Look Versus Evasive Glance and Compliance With A RequestDocument4 pagesDirect Look Versus Evasive Glance and Compliance With A RequestPublia PromenadeNo ratings yet
- Germ LayerDocument9 pagesGerm LayerJcee EsurenaNo ratings yet
- Press Release: Semarang, 22 October 2017 - PT Kalbe Farma TBK (Kalbe) Through Kalbe EthicalDocument2 pagesPress Release: Semarang, 22 October 2017 - PT Kalbe Farma TBK (Kalbe) Through Kalbe EthicalYessy YasmaraldaNo ratings yet
- Hearnshaw TSBE Conference Paper 2012Document8 pagesHearnshaw TSBE Conference Paper 2012FUCKUNo ratings yet
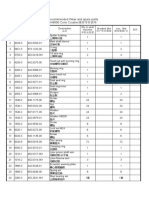
- Recommended Wear and spare parts H8800 Cone Crusher推荐零件清单Document3 pagesRecommended Wear and spare parts H8800 Cone Crusher推荐零件清单Lmf DanielNo ratings yet
- Plumber Faucets Price List 02.04.2022Document35 pagesPlumber Faucets Price List 02.04.2022rshaitansingh304No ratings yet
- Medication Errors PaperDocument6 pagesMedication Errors Paperapi-487459879No ratings yet
- Early Childhood Caries: Prevalence, Risk Factors, and PreventionDocument7 pagesEarly Childhood Caries: Prevalence, Risk Factors, and PreventioncareNo ratings yet
- Chlamydia InfectionsDocument4 pagesChlamydia InfectionsPearl CalisNo ratings yet
- Molybdenum Arene Final ReportDocument11 pagesMolybdenum Arene Final Reportapi-651962220No ratings yet
- Quiz Question 1 - MKSAP 17Document3 pagesQuiz Question 1 - MKSAP 17alaaNo ratings yet
- Quick Reference Handbook: B-HLF A330-342 MSN 0113Document262 pagesQuick Reference Handbook: B-HLF A330-342 MSN 0113mikeNo ratings yet
- Substance Abuse and Psychiatric: Disordersin Prison InmatesDocument3 pagesSubstance Abuse and Psychiatric: Disordersin Prison InmatesNorberth Ioan OkrosNo ratings yet
- Stroke Clinical PathwayDocument35 pagesStroke Clinical PathwayLaurencia Leny100% (2)
- Home Page Principles Practitioners Help Yourself Contact: Main NavigationDocument2 pagesHome Page Principles Practitioners Help Yourself Contact: Main NavigationAbdurrahmanUsmanNo ratings yet
- Kharif Crops Vs Rabi CropsDocument1 pageKharif Crops Vs Rabi CropsAsim MushtaqNo ratings yet
- Advanced Fire Fighting Course (5 Day) STCW-95Document2 pagesAdvanced Fire Fighting Course (5 Day) STCW-95hope earlNo ratings yet
- Indian Income Tax Return Acknowledgement 2021-22: Assessment YearDocument1 pageIndian Income Tax Return Acknowledgement 2021-22: Assessment YearPrateek GuptaNo ratings yet
- Teacher Attitudes Towards The Inclusion of Students With Support NeedsDocument10 pagesTeacher Attitudes Towards The Inclusion of Students With Support NeedsAndrej HodonjNo ratings yet