You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Anal Sex Secrets - A Guide To Great Anal Sex by Svetlana Ivanova - Read OnlineDocument4 pagesAnal Sex Secrets - A Guide To Great Anal Sex by Svetlana Ivanova - Read Onlinezamin4pak50% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eating Disorders: Anorexia Nervosa/Bulimia NervosaDocument15 pagesEating Disorders: Anorexia Nervosa/Bulimia NervosaCay Sevilla100% (8)
- Total Health Chapter 1,2 Review GameDocument123 pagesTotal Health Chapter 1,2 Review GameAlicia HigdonNo ratings yet
- Skin CareDocument5 pagesSkin Carejoseph100% (1)
- Head and NeckDocument21 pagesHead and NeckUday PrabhuNo ratings yet
- English Test: Surname: Points: /100Document3 pagesEnglish Test: Surname: Points: /100Елена Китанова ЃошевскаNo ratings yet
- Training Needs Assessment For NursesDocument3 pagesTraining Needs Assessment For NursesRodel Sumiran100% (1)
- Addison's DiseaseDocument17 pagesAddison's DiseaseMah Jezthy100% (1)
- Cleaning Validation Guidelines - Health CanadaDocument7 pagesCleaning Validation Guidelines - Health Canadahafeez50No ratings yet
- Humoral Innate Immunity and Acute-PhaseDocument14 pagesHumoral Innate Immunity and Acute-PhaseEdgar JoseNo ratings yet
- Effects of β blockers on all cause mortality in patients with diabetesDocument11 pagesEffects of β blockers on all cause mortality in patients with diabetesEsteban DavidNo ratings yet
- Malnutrition in Critical Illness and Beyond A Narrative Review PDFDocument9 pagesMalnutrition in Critical Illness and Beyond A Narrative Review PDFEsteban DavidNo ratings yet
- Aspirine Vs LMWH Nejm2023Document11 pagesAspirine Vs LMWH Nejm2023Esteban DavidNo ratings yet
- Osteoporosis 2020Document8 pagesOsteoporosis 2020Esteban DavidNo ratings yet
- Esc 2020Document15 pagesEsc 2020Esteban DavidNo ratings yet
- Jama Zampieri 2021 Oi 210083 1630095299.6909Document12 pagesJama Zampieri 2021 Oi 210083 1630095299.6909Esteban DavidNo ratings yet
- Heparin Beyond Anti-Coagulation: SciencedirectDocument4 pagesHeparin Beyond Anti-Coagulation: SciencedirectEsteban DavidNo ratings yet
- Ivermectin Covid 29Document20 pagesIvermectin Covid 29Esteban DavidNo ratings yet
- Hematuria en Adultos NEJM 2021Document11 pagesHematuria en Adultos NEJM 2021Esteban DavidNo ratings yet
- Letter - Mayor Johnson - 20181207Document2 pagesLetter - Mayor Johnson - 20181207Alyssa RobertsNo ratings yet
- Eye Drops and Dispensing Aids: A GuideDocument37 pagesEye Drops and Dispensing Aids: A GuideAamna ShahNo ratings yet
- Covid-19 Test Report: Patient Name: Akash GargDocument1 pageCovid-19 Test Report: Patient Name: Akash GargGenestrings Diagnostic CenterNo ratings yet
- Synerquest 2014 Annual Calendar of DOLE-prescribed CoursesDocument3 pagesSynerquest 2014 Annual Calendar of DOLE-prescribed CoursesrobinrubinaNo ratings yet
- Prevalence and Associated of Occular Morbidity in Luzira-UgandaDocument8 pagesPrevalence and Associated of Occular Morbidity in Luzira-Ugandadramwi edwardNo ratings yet
- Milarchi Lara Bulletin - Monthi Fest Issue, September 2022Document52 pagesMilarchi Lara Bulletin - Monthi Fest Issue, September 2022Kemmannu comNo ratings yet
- Pbs Register of SponsorsDocument1,727 pagesPbs Register of SponsorsZaili KastamNo ratings yet
- Full Length Research Article: ISSN: 2230-9926Document5 pagesFull Length Research Article: ISSN: 2230-9926Nisarg SutharNo ratings yet
- Topic: Use of Antibiotic Therapy For Pediatric Dental PatientsDocument1 pageTopic: Use of Antibiotic Therapy For Pediatric Dental PatientsTenzin WangyalNo ratings yet
- TGI0221 FinalDocument81 pagesTGI0221 FinalInes NarcisoNo ratings yet
- Assignment 15th BatchDocument2 pagesAssignment 15th Batchgagon-2021816127No ratings yet
- Speaking AVCN2Document6 pagesSpeaking AVCN22253010690No ratings yet
- Paaralang Sekundarya NG Lucban Integrated School: Research CapsuleDocument10 pagesPaaralang Sekundarya NG Lucban Integrated School: Research CapsuleJohn Lester M. Dela CruzNo ratings yet
- Effectiveness and Neural Mechanisms of Home-BasedDocument5 pagesEffectiveness and Neural Mechanisms of Home-BasedMuhammad ImronNo ratings yet
- Documents For Camp Attendance: I, Name....Document2 pagesDocuments For Camp Attendance: I, Name....Deva T N100% (1)
- Teva AR 2017 - PharmaceuticalIndustriesLtdDocument805 pagesTeva AR 2017 - PharmaceuticalIndustriesLtdBhushanNo ratings yet
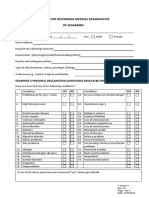
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- Kinjal AttachedDocument1 pageKinjal AttachedNilay JethavaNo ratings yet
- Staphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andDocument8 pagesStaphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andRisna IrvianiNo ratings yet
- What Is MastectomyDocument2 pagesWhat Is MastectomyMyami Bersamen100% (1)
- Carestream Quantum Medical Imaging QS 550 Tubestand DC30 034 RH 201506Document50 pagesCarestream Quantum Medical Imaging QS 550 Tubestand DC30 034 RH 201506D “DAKHobby” KNo ratings yet