You might also like
- Effects of Presession Pairing On Preference For Therapeutic ConditionsDocument6 pagesEffects of Presession Pairing On Preference For Therapeutic ConditionsNaia ArielNo ratings yet
- Summary of Ghana'S Nationally Appropriate Mitigation ActionsDocument25 pagesSummary of Ghana'S Nationally Appropriate Mitigation ActionsPrince AbokyeNo ratings yet
- Samuel Beckett - Dante... Bruno. Vico... JoyceDocument8 pagesSamuel Beckett - Dante... Bruno. Vico... JoyceLore Buchner100% (1)
- Pornography Addiction A Supranormal Stimulus Considered in The Context of NeuroplasticityDocument9 pagesPornography Addiction A Supranormal Stimulus Considered in The Context of NeuroplasticityTheodor IacobNo ratings yet
- 6733 FullDocument8 pages6733 FullGloopertNo ratings yet
- Nihms 1037223Document19 pagesNihms 1037223Helena OliveiraNo ratings yet
- Ajp 2007 164 1 4Document3 pagesAjp 2007 164 1 4Maritsa EngelbrechtNo ratings yet
- Working MemoryDocument9 pagesWorking MemoryIrene C. CruzNo ratings yet
- Lent 2012 PDFDocument4 pagesLent 2012 PDFBety Rafael PérezNo ratings yet
- Neurobiological Basis of HypersexualityDocument21 pagesNeurobiological Basis of HypersexualityUgur BuyuktezgelNo ratings yet
- Autonomous Motivation and Fruit-Vegetable Intake in Parent-Adolescent Dyads - Dwyer Et Al (2017)Document9 pagesAutonomous Motivation and Fruit-Vegetable Intake in Parent-Adolescent Dyads - Dwyer Et Al (2017)eaguirredNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptJohn SmithNo ratings yet
- 4 PDFDocument11 pages4 PDFHrishikesh BapatNo ratings yet
- 1 s2.0 S0079612315001909 MainDocument27 pages1 s2.0 S0079612315001909 Mainqnx22605No ratings yet
- 2016internationaljournalofhiv AidsandresearchDocument5 pages2016internationaljournalofhiv AidsandresearchAssyfa NoviaNo ratings yet
- Sensorimotor Gating, Orienting and Social Perception in SchizophreniaDocument7 pagesSensorimotor Gating, Orienting and Social Perception in SchizophreniaTsey IbrahimNo ratings yet
- C9a1 PDFDocument12 pagesC9a1 PDFfujfrNo ratings yet
- Neurobiology of AddictionDocument57 pagesNeurobiology of AddictionJef_8No ratings yet
- Howard 2020Document15 pagesHoward 2020andreaNo ratings yet
- Food Reward SystemDocument12 pagesFood Reward SystemCamilla MendesNo ratings yet
- Ni Hms 937807Document32 pagesNi Hms 937807Gilbert SihombingNo ratings yet
- Fall 2022 CultivateDocument15 pagesFall 2022 CultivateFlorida Horticulture for Health NetworkNo ratings yet
- 0-Addicto Craving Hone-Blanchet (2014)Document15 pages0-Addicto Craving Hone-Blanchet (2014)gildas5d5almeidaNo ratings yet
- Cognitive Neuroscience of 2018Document17 pagesCognitive Neuroscience of 2018Dhino Armand Quispe SánchezNo ratings yet
- Neurocognitive Underpinnings of Denial and Decision Making 1Document23 pagesNeurocognitive Underpinnings of Denial and Decision Making 1SARAHSTONGENo ratings yet
- Regular Activity DiabetesDocument10 pagesRegular Activity DiabetesDany RoaNo ratings yet
- Caspi Et Al - Genes and Its Influence On BehaviorDocument2 pagesCaspi Et Al - Genes and Its Influence On Behaviorlavannya aNo ratings yet
- Are You Morally EnhancedDocument16 pagesAre You Morally EnhancedSantiago CoboNo ratings yet
- Evidence-Based Pharmacotherapy For Personality DisordersDocument32 pagesEvidence-Based Pharmacotherapy For Personality Disordersibn SalamaNo ratings yet
- Clinical Psychology Review: Kathryn E. Smith, Tyler B. Mason, Jason M. LavenderDocument15 pagesClinical Psychology Review: Kathryn E. Smith, Tyler B. Mason, Jason M. LavenderLAURA CRISTINA TORRES CATANONo ratings yet
- Chew and SpitDocument7 pagesChew and SpitAlejandro Flores VelascoNo ratings yet
- Physical and Sexual Abuse Issues Among Youths With Substance Use ProblemsDocument5 pagesPhysical and Sexual Abuse Issues Among Youths With Substance Use Problemssondang simanjuntakNo ratings yet
- Castigo Físico y Desórdenes MentalesDocument11 pagesCastigo Físico y Desórdenes MentalesEduardo Espinoza GonzalesNo ratings yet
- Dissociation, Abuse and The Eating Disorders: Evidence From An Australian PopulationDocument8 pagesDissociation, Abuse and The Eating Disorders: Evidence From An Australian PopulationCoordinacionPsicologiaVizcayaGuaymasNo ratings yet
- Wood 2022 Sensory GI Issues Ver PDFDocument9 pagesWood 2022 Sensory GI Issues Ver PDFcLAUDIANo ratings yet
- Genetics IntroductionDocument2 pagesGenetics Introductionapi-188978784No ratings yet
- Ajp 155 4 479Document7 pagesAjp 155 4 479Lina RodríguezNo ratings yet
- Eating Disorders TheoryDocument9 pagesEating Disorders TheoryPayal MulaniNo ratings yet
- NeuralmarketingDocument9 pagesNeuralmarketingjbaksiNo ratings yet
- Mulligan2014 Article AnAnalysisOfTreatmentEfficacyFDocument22 pagesMulligan2014 Article AnAnalysisOfTreatmentEfficacyFPsicoterapia InfantilNo ratings yet
- Review: Conceptual Framework, Defi Nitions, and Animal ModelsDocument14 pagesReview: Conceptual Framework, Defi Nitions, and Animal ModelsMarinaNo ratings yet
- Self-Determination and Substance Use Is Effortful Control A MediatorDocument8 pagesSelf-Determination and Substance Use Is Effortful Control A Mediatorapi-463117687No ratings yet
- 1 s2.0 S0028390821001106 MainDocument29 pages1 s2.0 S0028390821001106 MainElisa RodríguezNo ratings yet
- Factors Affecting Addiction PDFDocument10 pagesFactors Affecting Addiction PDFLara MaxineNo ratings yet
- Emotional Development in Eating Disorders: A Qualitative Meta-SynthesisDocument41 pagesEmotional Development in Eating Disorders: A Qualitative Meta-SynthesisJulián SaugyNo ratings yet
- The Incentive Sensitization Theory of Addiction: Some Current Issues.Document10 pagesThe Incentive Sensitization Theory of Addiction: Some Current Issues.bonzosecoNo ratings yet
- Research PAPER Nguyen Thanh LongDocument16 pagesResearch PAPER Nguyen Thanh Longthaitoando510No ratings yet
- INHIBITIONDocument19 pagesINHIBITIONfranciscatomiNo ratings yet
- The Habitual Tendencies Questionnaire A Tool For PDocument17 pagesThe Habitual Tendencies Questionnaire A Tool For PRana KoshhaNo ratings yet
- Pathological Gambling and Substance Use Disorders: Justin D. Wareham, M.SCDocument6 pagesPathological Gambling and Substance Use Disorders: Justin D. Wareham, M.SCCoco AdarNo ratings yet
- Theories of Addiction: By-Manali Naphade (MA Psychology Sem III)Document24 pagesTheories of Addiction: By-Manali Naphade (MA Psychology Sem III)Manali NaphadeNo ratings yet
- Moelleretal 2001psychiatricaspectsofimpulsivityDocument12 pagesMoelleretal 2001psychiatricaspectsofimpulsivityZavršni radNo ratings yet
- Personality in Men With Eating DisordersDocument6 pagesPersonality in Men With Eating DisordersDANIEL PATRICK PALMA SEGOVIANo ratings yet
- A Randomized Controlled Trial of Group Reality TheDocument6 pagesA Randomized Controlled Trial of Group Reality TheValentina Arias MesaNo ratings yet
- Viewcontent CgiDocument38 pagesViewcontent Cgig.veraNo ratings yet
- Frontostriatal Circuits and The Development of Bulimia NervosaDocument12 pagesFrontostriatal Circuits and The Development of Bulimia NervosaShawna ChiewNo ratings yet
- Eye Tracking Research in Eating Disorders - A Systematic ReviewDocument25 pagesEye Tracking Research in Eating Disorders - A Systematic ReviewMirele Pereira de Aquino AlmeidaNo ratings yet
- FA of Aberrant Behavior Maintained by AFDocument15 pagesFA of Aberrant Behavior Maintained by AFAndrea Gallo de la PazNo ratings yet
- Neurobehavior & Special Sense System Tutor's Guide Substance Related DisorderDocument22 pagesNeurobehavior & Special Sense System Tutor's Guide Substance Related DisorderNovi AdriNo ratings yet
- Biological Substrates of Addiction 2014Document30 pagesBiological Substrates of Addiction 2014Jacky KarNo ratings yet
- Common MisconceptionsDocument1 pageCommon Misconceptionslet's skip thisNo ratings yet
- Audels Engineers and Mechanics Guide Volume 1 From WWW Jgokey ComDocument486 pagesAudels Engineers and Mechanics Guide Volume 1 From WWW Jgokey Comjdsa123100% (2)
- IRC-114-2013 Use of Silica Fume in Rigid PavementDocument14 pagesIRC-114-2013 Use of Silica Fume in Rigid PavementZakee MohamedNo ratings yet
- Intellectual Property Rights An IntroductionDocument140 pagesIntellectual Property Rights An IntroductionSumatthi Devi ChigurupatiNo ratings yet
- FlywheelDocument2 pagesFlywheelSaravanan MathiNo ratings yet
- LagundiDocument4 pagesLagundiAileen A. MonaresNo ratings yet
- H1M Series ManualDocument13 pagesH1M Series Manualmiguel brunoNo ratings yet
- Reviewer For Practical Research 1 PrelimDocument5 pagesReviewer For Practical Research 1 PrelimMaureen ElumbaringNo ratings yet
- (CASS Series - Naval Policy and History 62) Milan Vego - Maritime Strategy and Sea Denial - Theory and Practice-Routledge (2019)Document349 pages(CASS Series - Naval Policy and History 62) Milan Vego - Maritime Strategy and Sea Denial - Theory and Practice-Routledge (2019)akun bebaz100% (1)
- Role of Observational Medicine in EmergencyDocument13 pagesRole of Observational Medicine in EmergencyazhaabazNo ratings yet
- Additives For Adhesives and Sealants Catalogue EuropeDocument24 pagesAdditives For Adhesives and Sealants Catalogue EuropeAlexi WiedemannNo ratings yet
- Skpi Astri BelindaDocument7 pagesSkpi Astri BelindaDewakopa FNo ratings yet
- The Misconception About Radiologic Technology Regarding The Effects of Radiation in Reproductive Health. SynthesisDocument4 pagesThe Misconception About Radiologic Technology Regarding The Effects of Radiation in Reproductive Health. SynthesisCathleen Drew TuazonNo ratings yet
- Chapter 1 - MEDocument10 pagesChapter 1 - MEMd. Azmain AdilNo ratings yet
- Mitosis: Aarifa Hoosein-RiyasatDocument28 pagesMitosis: Aarifa Hoosein-RiyasatAkiela JohnsonNo ratings yet
- PlumsDocument17 pagesPlumsM.P. SeenivasanNo ratings yet
- Alexander Technique and ActingDocument33 pagesAlexander Technique and ActingatsteNo ratings yet
- Azerbaijan Renewable EnergyDocument20 pagesAzerbaijan Renewable EnergyAhmed Imtiaz RaoNo ratings yet
- Attachment-02 Catalog PDFDocument85 pagesAttachment-02 Catalog PDFKais MessaoudiNo ratings yet
- Erikson Daily Report 14 JanuaryDocument12 pagesErikson Daily Report 14 Januaryrizal355No ratings yet
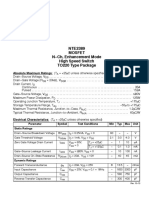
- NTE2389 Mosfet N CH, Enhancement Mode High Speed Switch TO220 Type PackageDocument2 pagesNTE2389 Mosfet N CH, Enhancement Mode High Speed Switch TO220 Type PackagetoroalNo ratings yet
- Kronig Penney ModelDocument3 pagesKronig Penney ModelHolloGramNo ratings yet
- L03B-Dimensional Modeling IIDocument36 pagesL03B-Dimensional Modeling IIFrans SitohangNo ratings yet
- Quiz 1Document2 pagesQuiz 1Jun RyNo ratings yet
- C1036 16Document10 pagesC1036 16masoudNo ratings yet
- Portfolio Ende2011 WebDocument37 pagesPortfolio Ende2011 WebJörn LutterNo ratings yet
- AlbuminuriaDocument3 pagesAlbuminuriaAyunda Aura SalsabilNo ratings yet
- The The: Evolution of Warren, or Triangular, TrussDocument1 pageThe The: Evolution of Warren, or Triangular, TrussMr. DreamNo ratings yet