You might also like
- Vitamin D Deficiency: Epidemiology, Pathophysiology and ManagementDocument61 pagesVitamin D Deficiency: Epidemiology, Pathophysiology and ManagementSalmanNo ratings yet
- AB in HematooncoDocument39 pagesAB in HematooncokemalahmadNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- Niv HFNCDocument15 pagesNiv HFNCFrank VaronaNo ratings yet
- BronchiolitisDocument17 pagesBronchiolitisRizky DarmawanNo ratings yet
- Nippv Revisi Final Picu Nicu MaretDocument51 pagesNippv Revisi Final Picu Nicu MaretJulian Ammar Zaidan GunawanNo ratings yet
- Gagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanDocument20 pagesGagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanAdlan BinharyantoNo ratings yet
- Obesity in ChildrenDocument15 pagesObesity in ChildrenJohn ConnorNo ratings yet
- Childhood ObesityDocument70 pagesChildhood ObesityMedical SuperintendentNo ratings yet
- Sindroma Metabolik Dislipidemia Dan ObesitasDocument45 pagesSindroma Metabolik Dislipidemia Dan ObesitasLaurentius Juan WicaksonoNo ratings yet
- Ringer Asetat Pada AnakDocument72 pagesRinger Asetat Pada Anaknanda surastyo100% (1)
- Pneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsDocument34 pagesPneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsMenard Velasco100% (1)
- Meconium Aspiration: Ospital NG Maynila Medical Center Department of PediatricsDocument38 pagesMeconium Aspiration: Ospital NG Maynila Medical Center Department of PediatricsGrace Antonette Pati100% (1)
- Sepsis Induced CholestasisDocument12 pagesSepsis Induced CholestasisYusuf Hakim AjiNo ratings yet
- MeningitisDocument20 pagesMeningitisAmalia Tri UtamiNo ratings yet
- Meningitis Bacteriana y Viral 3Document15 pagesMeningitis Bacteriana y Viral 3María Nurys Acevedo CerchiaroNo ratings yet
- Dyspnea in Children - Wahyuni IndawatiDocument20 pagesDyspnea in Children - Wahyuni IndawatiTarmidi MidziNo ratings yet
- Dampak Jangka Panjang StuntingDocument37 pagesDampak Jangka Panjang StuntingFina GisnawatyNo ratings yet
- PAT + Primary SurveyDocument33 pagesPAT + Primary Surveysalsa100% (1)
- ATI Med Surg SPRING 2019 Post ReviewDocument11 pagesATI Med Surg SPRING 2019 Post ReviewQuincey Hamilton43% (7)
- 03 - DR - Dominicus - PELATIHAN DIFTERI SMD 17 Jan 2018 - Diagnosis - SharedDocument54 pages03 - DR - Dominicus - PELATIHAN DIFTERI SMD 17 Jan 2018 - Diagnosis - SharedFebria Valentine AritonangNo ratings yet
- Jurnal RabiesDocument19 pagesJurnal RabiesjenifermtNo ratings yet
- DEN GU E: DengueDocument53 pagesDEN GU E: Denguerose ONo ratings yet
- Batuk Kronik BerulangDocument24 pagesBatuk Kronik BerulangHameldo Andika PattinasaranyNo ratings yet
- Impaired Gas ExchangeDocument5 pagesImpaired Gas ExchangeKM67% (3)
- NBS Law FinalDocument33 pagesNBS Law Finalkissiah Cajetas100% (1)
- High Flow Nasal Cannula and Humidification: Nick Dalmon Staff Nurse Intensive Care, William Harvey HospitalDocument23 pagesHigh Flow Nasal Cannula and Humidification: Nick Dalmon Staff Nurse Intensive Care, William Harvey HospitalMori ArisandyNo ratings yet
- Types of Developmental DisordersDocument60 pagesTypes of Developmental DisordersAnshika ChaudhryNo ratings yet
- PPT Referat ADHD - Kevin LukitoDocument22 pagesPPT Referat ADHD - Kevin LukitonoviaNo ratings yet
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- Ventilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMDocument52 pagesVentilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMireneaureliaNo ratings yet
- Kuliah BBLR PrematurDocument28 pagesKuliah BBLR PrematurafraxyzNo ratings yet
- Perinatal Asphyxia: Walter Otieno Consultant PaediatricianDocument25 pagesPerinatal Asphyxia: Walter Otieno Consultant PaediatricianMalueth AnguiNo ratings yet
- MalariaDocument23 pagesMalariaIBhe Damianry QritezzNo ratings yet
- Japanese EncephalitisDocument14 pagesJapanese EncephalitisMuhammad Rafli AkbarNo ratings yet
- 2017 Tubulointerstitial Nephritis, Diagnosis, Treatment, and MonitoringDocument11 pages2017 Tubulointerstitial Nephritis, Diagnosis, Treatment, and MonitoringbrufenNo ratings yet
- Kuliah Pengayaan DM 2017-1Document100 pagesKuliah Pengayaan DM 2017-1Syarifah Maharani HidayatNo ratings yet
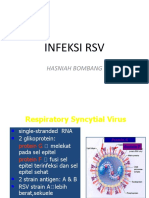
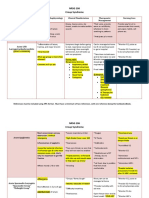
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahNo ratings yet
- 02NTD 2022 - Approach To Severe DengueDocument54 pages02NTD 2022 - Approach To Severe DengueInstitute for Clinical ResearchNo ratings yet
- Effect of Ursodeoxycholic Acid On Indirect Hyperbilirubinemia in Neonates Treated With PhototherapyDocument4 pagesEffect of Ursodeoxycholic Acid On Indirect Hyperbilirubinemia in Neonates Treated With PhototherapyEka Satria AnanditaNo ratings yet
- Syok Pada AnakDocument28 pagesSyok Pada AnakTaufik Abidin100% (1)
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiNo ratings yet
- Larsen Syndrome: - Dr. Kapil R JagtapDocument23 pagesLarsen Syndrome: - Dr. Kapil R JagtapKapil JagtapNo ratings yet
- Referat ObesitasDocument20 pagesReferat ObesitasfaisalNo ratings yet
- PPT DIARHEA IN CHILDRENDocument31 pagesPPT DIARHEA IN CHILDRENRifka AnisaNo ratings yet
- Obesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Document27 pagesObesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Andrie WigunaNo ratings yet
- Hospital PneumoniaDocument12 pagesHospital PneumoniaKartika RezkyNo ratings yet
- Case AnakDocument28 pagesCase AnakAmorrita Puspita RatuNo ratings yet
- Bronkopneumonia Pada Pasien PediatrikDocument5 pagesBronkopneumonia Pada Pasien PediatrikCecilia Evangelista NiluhNo ratings yet
- MedulloblastomaDocument67 pagesMedulloblastomaAmira YasmineNo ratings yet
- Cerebral Toxoplasmosis: Diagnosis & ManagementDocument32 pagesCerebral Toxoplasmosis: Diagnosis & ManagementShinta DianNo ratings yet
- Atelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Document5 pagesAtelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Renato Li SoldevillaNo ratings yet
- Pituitary Adenomas in Adolescence Diagnostic Approach and Therapeutic Strategy GarofaloDocument48 pagesPituitary Adenomas in Adolescence Diagnostic Approach and Therapeutic Strategy GarofaloClaudia IrimieNo ratings yet
- NRSG 206 Croup SyndromeDocument3 pagesNRSG 206 Croup SyndromeGirlwithnonameNo ratings yet
- Faltering Growth: Straight To The Point of CareDocument35 pagesFaltering Growth: Straight To The Point of Careftah ahmedNo ratings yet
- Neurodermatitis (Lichen Simplex Chronic)Document26 pagesNeurodermatitis (Lichen Simplex Chronic)Yusran Ady FitrahNo ratings yet
- Neonatal Infection: Julniar M Tasli Herman Bermawi Afifa RamadantiDocument56 pagesNeonatal Infection: Julniar M Tasli Herman Bermawi Afifa RamadantiOtchi Pudtrie WijayaNo ratings yet
- Approach To Child With WheezingpediatricsDocument25 pagesApproach To Child With WheezingpediatricsshahinaNo ratings yet
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Document46 pages1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริNo ratings yet
- Stunting (EDIT)Document62 pagesStunting (EDIT)846035No ratings yet
- Early Assessment of Respiratory DistressDocument17 pagesEarly Assessment of Respiratory DistressRosi AmaliaNo ratings yet
- High-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningDocument3 pagesHigh-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningMahmoud khedrNo ratings yet
- Lecture Anwar Ventilation Managment COVIDDocument28 pagesLecture Anwar Ventilation Managment COVIDمحمدرزازالتبعيNo ratings yet
- PPHN Edit 17-FebDocument38 pagesPPHN Edit 17-FebAlbert GunawanNo ratings yet
- 2023 The Sanford Guide - PDFDocument40 pages2023 The Sanford Guide - PDFMinodora FaurNo ratings yet
- Sepsis and Septic Shock - Critical Care MedicineDocument2 pagesSepsis and Septic Shock - Critical Care MedicineMihaela MoraruNo ratings yet
- Hipoxemia RefratariaDocument4 pagesHipoxemia RefratariaThiago LacerdaNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- ABG BASICS YvonneDocument48 pagesABG BASICS Yvonneนีล ไบรอันNo ratings yet
- TERAPI OKSIGEN (Basic: Binasal Dan Facemask) PDFDocument43 pagesTERAPI OKSIGEN (Basic: Binasal Dan Facemask) PDFchristintinneNo ratings yet
- Statement On Pulmonary RehabilitationDocument24 pagesStatement On Pulmonary RehabilitationDavidMorenoTovarNo ratings yet
- Oxygenation, Oxygen Delivery and Anaesthesia in The Horse: J. A. E. Hubbell and W. W. MuirDocument11 pagesOxygenation, Oxygen Delivery and Anaesthesia in The Horse: J. A. E. Hubbell and W. W. MuirGuillermo GpNo ratings yet
- N118 0XYGEN Checklist FinalDocument7 pagesN118 0XYGEN Checklist FinalAmandaNo ratings yet
- Basics in Arterial Blood Gas InterpretationDocument41 pagesBasics in Arterial Blood Gas InterpretationyasinNo ratings yet
- Pharmacological Management ofDocument9 pagesPharmacological Management ofAishah FarihaNo ratings yet
- Adjuncts To Mechanical Ventilation: Tantani SugimanDocument36 pagesAdjuncts To Mechanical Ventilation: Tantani SugimanAndi Upik FathurNo ratings yet
- 312 - ABG Analysis & IV Therapy and MedicationDocument5 pages312 - ABG Analysis & IV Therapy and MedicationFRANCINE EVE ESTRELLANNo ratings yet
- High Altitude Phisiology: Adiartha GriadhiDocument43 pagesHigh Altitude Phisiology: Adiartha GriadhilindaNo ratings yet
- HypoxemiaDocument3 pagesHypoxemiaMark Angelo ChanNo ratings yet
- Guía OxigenoterapiaDocument39 pagesGuía OxigenoterapiaSMIBA MedicinaNo ratings yet
- Acute Respiratory FailureDocument72 pagesAcute Respiratory Failureraghad awwadNo ratings yet
- CMO 09 s2007Document55 pagesCMO 09 s2007XtiaRNo ratings yet
- Hypoxia: Symptoms: Its Causes andDocument5 pagesHypoxia: Symptoms: Its Causes andRosihayati100% (1)
- Eng 2006 MedDocument43 pagesEng 2006 MedLucia BogNo ratings yet
- Respiratory MS NOTESDocument15 pagesRespiratory MS NOTESMARY ANN CAGATANNo ratings yet
- Therapy: Dr. Ravinder Narwal MPT Cardiopulmonary MPT-OrthoDocument27 pagesTherapy: Dr. Ravinder Narwal MPT Cardiopulmonary MPT-OrthoRavin NarwalNo ratings yet
- Respiratory FailureDocument29 pagesRespiratory Failureageng rusbaya0% (1)
- Preparing MedicationsDocument18 pagesPreparing MedicationsJuliezel IringanNo ratings yet
- Final Content ET Intubation 1Document27 pagesFinal Content ET Intubation 1Debipriya MistryNo ratings yet
- CHPT 70 Respiratory Part 2Document56 pagesCHPT 70 Respiratory Part 2helen brockNo ratings yet