100% found this document useful (3 votes)
4K views1 pagePeripheral I.V. Line Checklist (Visual Infusion Phlebitis Score)
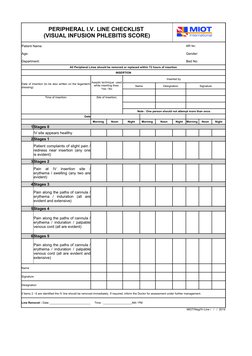
This document provides a checklist for monitoring peripheral intravenous (IV) lines using the Visual Infusion Phlebitis Score. The checklist collects patient information and details of IV line insertion including date, time, site and person who inserted the line. Nurses then assess and document the condition of the IV site each morning, noon and night using a 6 stage scale. Lines showing signs of infection or inflammation from stages 2-6 should be immediately removed and the doctor informed. The date and time of any line removal is also recorded.
Uploaded by
aashika15Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
100% found this document useful (3 votes)
4K views1 pagePeripheral I.V. Line Checklist (Visual Infusion Phlebitis Score)
This document provides a checklist for monitoring peripheral intravenous (IV) lines using the Visual Infusion Phlebitis Score. The checklist collects patient information and details of IV line insertion including date, time, site and person who inserted the line. Nurses then assess and document the condition of the IV site each morning, noon and night using a 6 stage scale. Lines showing signs of infection or inflammation from stages 2-6 should be immediately removed and the doctor informed. The date and time of any line removal is also recorded.
Uploaded by
aashika15Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
- Peripheral I.V. Line Checklist