You might also like
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- Complaint-Affidavit Intriguing Against HonorDocument2 pagesComplaint-Affidavit Intriguing Against HonorConsigliere Tadili75% (4)
- Hesi RN Exit Exam V3Document37 pagesHesi RN Exit Exam V3Eniti100% (1)
- Blood CollectionDocument120 pagesBlood CollectionDan Mikhail TingubanNo ratings yet
- Emergency and Disaster NursingDocument17 pagesEmergency and Disaster NursingKoleen Kirsten67% (3)
- Multiple Choice Questions in Paediatric SurgeryFrom EverandMultiple Choice Questions in Paediatric SurgeryRating: 1 out of 5 stars1/5 (1)
- Er 1Document8 pagesEr 1Justin HannahNo ratings yet
- NCP PcapDocument2 pagesNCP PcapGacutan Jonathan88% (25)
- Med SurgDocument23 pagesMed SurgReymart AcalaNo ratings yet
- Compre - NP 3 Ans. KeyDocument13 pagesCompre - NP 3 Ans. KeyJune Dumdumaya100% (2)
- 01 Intro To TCCC For All Combatants 140602Document53 pages01 Intro To TCCC For All Combatants 140602Bruno100% (1)
- Emergency Nursing Board Exam Review QuestionsDocument17 pagesEmergency Nursing Board Exam Review QuestionsAlsalman AnamNo ratings yet
- EMERGENCY ROOM CAREDocument33 pagesEMERGENCY ROOM CAREJillian EsquivelNo ratings yet
- Neonatal and Pediatric Respiratory Care 5th EditionDocument61 pagesNeonatal and Pediatric Respiratory Care 5th Editioneleanor.gamble412100% (45)
- Nursing Board Exam Review Questions in Emergency Part 6/20Document15 pagesNursing Board Exam Review Questions in Emergency Part 6/20Tyron Rigor Silos100% (5)
- Ms Emergency Disaster Preparedness-J11-212 UpdtdDocument5 pagesMs Emergency Disaster Preparedness-J11-212 UpdtdyusiviNo ratings yet
- Er Test DrillsDocument26 pagesEr Test DrillsconinitasNo ratings yet
- Nursing Care for Terminally Ill Patients and Their FamiliesDocument7 pagesNursing Care for Terminally Ill Patients and Their FamiliesMarie Jhoana100% (1)
- Pediatric Nursing Questions on Meningitis, Isolation Precautions, Burns and MoreDocument22 pagesPediatric Nursing Questions on Meningitis, Isolation Precautions, Burns and MoreDarren Flores100% (1)
- Bacteriotherapy Faqs PDFDocument17 pagesBacteriotherapy Faqs PDFpavaroti37No ratings yet
- Pre Board ResultsDocument28 pagesPre Board ResultsMichael MontañoNo ratings yet
- Compre - ExamDocument12 pagesCompre - ExamJet Padamada50% (2)
- Ipi Nursing Part 1,2,3Document53 pagesIpi Nursing Part 1,2,3Noleen MckayNo ratings yet
- Sample Questions For HAAD Prometric and DHA For NursesDocument46 pagesSample Questions For HAAD Prometric and DHA For NursesJaezelle Ella Sabale100% (4)
- Comprehensive Exam 1Document19 pagesComprehensive Exam 1karenkaren09100% (1)
- Medical Emergencies in Early Childhood and School-Age SettingsFrom EverandMedical Emergencies in Early Childhood and School-Age SettingsNo ratings yet
- PNLE Maternal and Child Health Nursing Exam 3Document29 pagesPNLE Maternal and Child Health Nursing Exam 3Denisse Palay100% (1)
- Emergency Nclex QuestionsDocument19 pagesEmergency Nclex QuestionsAlsalman Anam100% (8)
- Set III. Care of Clients With Physiologic and Psychosocial Alterations A (Answers)Document9 pagesSet III. Care of Clients With Physiologic and Psychosocial Alterations A (Answers)Yaj Cruzada100% (6)
- Emergency Room QuestionsDocument5 pagesEmergency Room QuestionsCharles Anthony Lopez EstebanNo ratings yet
- CHAPTER 16 MEDICAL Û SURGICAL EMERGENCIESDocument10 pagesCHAPTER 16 MEDICAL Û SURGICAL EMERGENCIESjev_belardoNo ratings yet
- ED Nursing Assignments & PrioritizationDocument9 pagesED Nursing Assignments & PrioritizationVivian Montesena Breganza100% (1)
- NPT 3Document8 pagesNPT 3chrizthineeNo ratings yet
- Ed QuestionsDocument5 pagesEd Questionsherbert100% (1)
- NP4 Nursing Board ExamDocument5 pagesNP4 Nursing Board ExamNewb TobikkoNo ratings yet
- CBT Practice QuizDocument37 pagesCBT Practice QuizAnderson Alfred69% (13)
- Practice Questions - EDNDocument6 pagesPractice Questions - EDNKaren BlancoNo ratings yet
- جراحة - خالد الهبيل 8Document5 pagesجراحة - خالد الهبيل 8hasan ahmdNo ratings yet
- NCM 417 - Final Exam 2014Document12 pagesNCM 417 - Final Exam 2014Mae DacerNo ratings yet
- GFSDGSDGFSDGDocument2 pagesGFSDGSDGFSDGMA IZNo ratings yet
- Practice Test Questions MsDocument5 pagesPractice Test Questions MsRommel Joseph DionoraNo ratings yet
- 12Document13 pages12Mhia Mhi-mhi FloresNo ratings yet
- Homework Task 1Document10 pagesHomework Task 1Alyxen PelingenNo ratings yet
- Diagnostic ExaminationDocument10 pagesDiagnostic ExaminationHain YoloNo ratings yet
- نقابة التمريض الفلسطينية 7Document11 pagesنقابة التمريض الفلسطينية 7أبوأحمد الحكيمNo ratings yet
- Funda QuizDocument7 pagesFunda Quizgunn twothingNo ratings yet
- PRACTICE TEST 1 - SECE StudentDocument17 pagesPRACTICE TEST 1 - SECE StudentAlex OlivarNo ratings yet
- Exam 4 PDFDocument10 pagesExam 4 PDFأحمد المصريNo ratings yet
- CDC TesmanshipDocument33 pagesCDC TesmanshipCamille GalasNo ratings yet
- Nursing Care Management ExamDocument29 pagesNursing Care Management Examimyutheyu07No ratings yet
- NCLEX Practice Test: Nursing Care of ChildrenDocument55 pagesNCLEX Practice Test: Nursing Care of ChildrenNicholas TagleNo ratings yet
- Fundamentals Of: NursingDocument15 pagesFundamentals Of: NursingJanreyQuesioMiñaoNo ratings yet
- II MOCK TEST Questions OnlyDocument46 pagesII MOCK TEST Questions OnlyazitaaaaaNo ratings yet
- NP 1 To 5 Focus210-D WITHOUT AnswersDocument5 pagesNP 1 To 5 Focus210-D WITHOUT AnswersMarkie CubosNo ratings yet
- Post Test 2 RationalesDocument11 pagesPost Test 2 Rationalesrhymes2u100% (2)
- Prometric QR7 2Document11 pagesPrometric QR7 2tqmgkx7p8rNo ratings yet
- Preboard 28 BDocument7 pagesPreboard 28 BRakeem MarquiseNo ratings yet
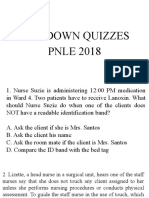
- Sundown Quizzes PNLE 2018Document42 pagesSundown Quizzes PNLE 2018Mon DoceNo ratings yet
- Care For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19From EverandCare For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19No ratings yet
- Care For Vulnerable Populations During COVID-19 PandemicFrom EverandCare For Vulnerable Populations During COVID-19 PandemicNo ratings yet
- Introduction To Problem Solving in The Information Age: Lesson 1 - New Learning Skills 2Document8 pagesIntroduction To Problem Solving in The Information Age: Lesson 1 - New Learning Skills 2hayleykhoNo ratings yet
- Child and Adolescent Development Research Module 4Document15 pagesChild and Adolescent Development Research Module 4Michelle Joy M. VicenteNo ratings yet
- Module 3 Michelle Joy VicenteDocument7 pagesModule 3 Michelle Joy VicenteMichelle Joy M. VicenteNo ratings yet
- Sample Gap LetterDocument1 pageSample Gap LetterMichelle Joy M. VicenteNo ratings yet
- 19 Prenatal and Antepartum ManagementDocument34 pages19 Prenatal and Antepartum ManagementMichelle Joy M. VicenteNo ratings yet
- 16 Medication AdministrationDocument26 pages16 Medication AdministrationMichelle Joy M. VicenteNo ratings yet
- 15 Basic Care and ComfortDocument24 pages15 Basic Care and ComfortMichelle Joy M. VicenteNo ratings yet
- 13 Safety Accident Injury and Error PreventionDocument23 pages13 Safety Accident Injury and Error PreventionMichelle Joy M. VicenteNo ratings yet
- 14 Infection ControlDocument27 pages14 Infection ControlMichelle Joy M. VicenteNo ratings yet
- Basic Information On Pharmaceutical Dosage Forms and Drug Delivery SystemsDocument30 pagesBasic Information On Pharmaceutical Dosage Forms and Drug Delivery SystemsSyed Hussain AsafNo ratings yet
- List New Cath LabDocument3 pagesList New Cath LabtazkiaNo ratings yet
- Abbrivation of Medical TrminologyDocument1,215 pagesAbbrivation of Medical Trminologyapi-271694220No ratings yet
- El PsaDocument2 pagesEl PsaMaherNo ratings yet
- Stok SDM 02 01 23Document6 pagesStok SDM 02 01 23Lilis EkaNo ratings yet
- Microbiologia de Murray 8va Edicion-194-227Document34 pagesMicrobiologia de Murray 8va Edicion-194-227Ailyn Montalvo FigueroaNo ratings yet
- Trauma Final Exam QuestionsDocument155 pagesTrauma Final Exam QuestionsElo GonçalvesNo ratings yet
- Position Paper: A B C D e F G H CDocument11 pagesPosition Paper: A B C D e F G H CNico IonaşcuNo ratings yet
- RCT - Masters - 2022Document24 pagesRCT - Masters - 2022Kanwal KhanNo ratings yet
- Feu GP FGTDocument16 pagesFeu GP FGTAla'a Emerald AguamNo ratings yet
- Dengue (Lancet)Document16 pagesDengue (Lancet)Roberth Mero100% (1)
- DesoxypipradrolDocument4 pagesDesoxypipradrolMarcNo ratings yet
- Tricat Trio InsertDocument2 pagesTricat Trio InsertSumanta MannaNo ratings yet
- Drug inventory listDocument2 pagesDrug inventory listEdwin SartorioNo ratings yet
- Fluid and Electrolyte Therapy for Pets with Vomiting and DiarrheaDocument22 pagesFluid and Electrolyte Therapy for Pets with Vomiting and Diarrheafernin96No ratings yet
- ACOG Practice Bulletin No 202Document25 pagesACOG Practice Bulletin No 202Berri RahmadhoniNo ratings yet
- BAPES 2021: The Annual Meeting of The British Association of Paediatric Endoscopic SurgeonsDocument10 pagesBAPES 2021: The Annual Meeting of The British Association of Paediatric Endoscopic SurgeonsRho GarNo ratings yet
- RT PCRDocument24 pagesRT PCRJhasmine GañalonNo ratings yet
- Vocabulary For Med InterpreterDocument6 pagesVocabulary For Med InterpreterSantiago Ardila-CortesNo ratings yet
- Osteoarthritis and GoutDocument69 pagesOsteoarthritis and Goutadamu mohammadNo ratings yet
- Benzo ZdrugDocument12 pagesBenzo Zdruglnair_43No ratings yet
- Bactec Mgit 960 CultureDocument15 pagesBactec Mgit 960 CultureKanzlerin UrielNo ratings yet
- Phs Mammographer PresentationDocument10 pagesPhs Mammographer Presentationapi-546893338No ratings yet
- StreptomycinDocument1 pageStreptomycinDemilyn Fat100% (2)
- NTP MOP 6th Ed Module 7 Treatment of TB in Special Situations 10.20.20Document56 pagesNTP MOP 6th Ed Module 7 Treatment of TB in Special Situations 10.20.20gbNo ratings yet