You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Contoh Kasus MCTDDocument3 pagesContoh Kasus MCTDElva KadarhadiNo ratings yet
- Ijcri - 201409ab - Full - Issue Hal 650Document71 pagesIjcri - 201409ab - Full - Issue Hal 650Elva KadarhadiNo ratings yet
- Brito - Chromoblastomycosis An Etiological, Epidemiological, Clinical, Diagnostic, and Treatment UpdateDocument12 pagesBrito - Chromoblastomycosis An Etiological, Epidemiological, Clinical, Diagnostic, and Treatment UpdateElva KadarhadiNo ratings yet
- Bonifaz A - Cutaneous Disseminated and Extracutaneous Sporotrichosis Current Status of A Complex Disease.Document13 pagesBonifaz A - Cutaneous Disseminated and Extracutaneous Sporotrichosis Current Status of A Complex Disease.Elva KadarhadiNo ratings yet
- Al-Kathiri - Uccessful Treatment of Recalcitrant Actinomycetoma of Gluteal Area With Combined Medical TreatmentDocument5 pagesAl-Kathiri - Uccessful Treatment of Recalcitrant Actinomycetoma of Gluteal Area With Combined Medical TreatmentElva KadarhadiNo ratings yet
- Azhar Hamed Gatea - Review On Analysis of Interesting Whitening Agents in Cosmetics ProductsDocument9 pagesAzhar Hamed Gatea - Review On Analysis of Interesting Whitening Agents in Cosmetics ProductsElva KadarhadiNo ratings yet
- Systematic Review of Platelet-Rich Plasma Use in Androgenetic Alopecia Compared With Minoxidil, Finasteride and Adult Stem Cell Based TherapyDocument26 pagesSystematic Review of Platelet-Rich Plasma Use in Androgenetic Alopecia Compared With Minoxidil, Finasteride and Adult Stem Cell Based TherapyElva KadarhadiNo ratings yet
- Review Article: Systemic Glutathione As A Skin-Whitening Agent in AdultDocument6 pagesReview Article: Systemic Glutathione As A Skin-Whitening Agent in AdultElva KadarhadiNo ratings yet
- TLC Flyer AADocument8 pagesTLC Flyer AAbearteddy17193No ratings yet
- Introduction To Dermatology: Lecture-1Document33 pagesIntroduction To Dermatology: Lecture-1Latika ChoudhuryNo ratings yet
- PDF CropDocument6 pagesPDF Crop04vijilNo ratings yet
- Patient Satisfaction PDFDocument5 pagesPatient Satisfaction PDFBîrlădeanu Ramona ElenaNo ratings yet
- Bonus CBO Master ProductsDocument94 pagesBonus CBO Master ProductsCarol GuzmánNo ratings yet
- THALIONDocument2 pagesTHALIONAjurs UrsabiaNo ratings yet
- Report Pilar 07 Maret 2022Document21 pagesReport Pilar 07 Maret 2022Haerul AkbarNo ratings yet
- Discoloration Correcting SerumDocument1 pageDiscoloration Correcting SerumfreemailtouseorwtvrNo ratings yet
- Skin Lesions SummaryDocument6 pagesSkin Lesions Summarypattydump11No ratings yet
- Generic Skin Care Questionnaire 1Document2 pagesGeneric Skin Care Questionnaire 1João Pedro AraújoNo ratings yet
- Lebanese DoctorsDocument2 pagesLebanese DoctorsmonicafernandesNo ratings yet
- Country's First Super Specialized Hospital at BSMMUDocument3 pagesCountry's First Super Specialized Hospital at BSMMUtanzim ornabNo ratings yet
- Theory Lesson Plan - Kylah Cla-3Document13 pagesTheory Lesson Plan - Kylah Cla-3claytonca19No ratings yet
- Team AppndDocument114 pagesTeam AppndGrc hashtagNo ratings yet
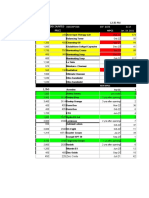
- Regular Discounted Price Price: Descripti0N Exp. Date As of Jan. 14, 2021Document1 pageRegular Discounted Price Price: Descripti0N Exp. Date As of Jan. 14, 2021Angela ReyesNo ratings yet
- E Brosur NMW Clinic 2022 PDFDocument29 pagesE Brosur NMW Clinic 2022 PDFAlpha OmegaNo ratings yet
- Katalog Skincare A4 Bagi 2Document1 pageKatalog Skincare A4 Bagi 2Jamal JppNo ratings yet
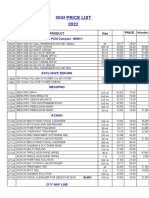
- Gigi Price List UusDocument7 pagesGigi Price List UusГалинаNo ratings yet
- Service Marketing Assignment: Submitted by Zain Raza (M19107)Document8 pagesService Marketing Assignment: Submitted by Zain Raza (M19107)hrushiNo ratings yet
- Thesis Done in DermatologyDocument7 pagesThesis Done in DermatologyWriteMyPaperForMeCheapCanada100% (2)
- Get Rid of Pimple in Four Easy StepsDocument20 pagesGet Rid of Pimple in Four Easy StepsOttah BlessingNo ratings yet
- Httpslumenis - Itwp Contentuploads201807PB 1000120 Rev.a IPL Bibliography For Print PDFDocument48 pagesHttpslumenis - Itwp Contentuploads201807PB 1000120 Rev.a IPL Bibliography For Print PDFUmberto Lo PassoNo ratings yet
- Trial 2Document2 pagesTrial 2Jayzelle Anne de LeonNo ratings yet
- Multi-Mechanism Skin Brightening Sabi WhiteDocument6 pagesMulti-Mechanism Skin Brightening Sabi WhiteMuhammad Akhyar RosyidiNo ratings yet
- Pore Strips For Black Heads - Google SearchDocument1 pagePore Strips For Black Heads - Google SearchcomingsooncomingbackNo ratings yet
- Analisa Asam SalisilatDocument5 pagesAnalisa Asam SalisilatMahardikaNo ratings yet
- ENERPEEL PA - Rev - 0 - 2011Document33 pagesENERPEEL PA - Rev - 0 - 2011CHONG WEI SHENGNo ratings yet
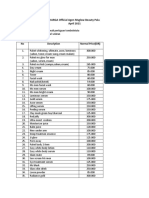
- HARGA Official Agen Msglow Beauty PaluDocument2 pagesHARGA Official Agen Msglow Beauty PaluAgung IcuNo ratings yet
- Pressure Ulcer StagesDocument3 pagesPressure Ulcer Stagesfreemind323No ratings yet
- 1300 2971 1 SMDocument9 pages1300 2971 1 SMserlinNo ratings yet