You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Oxford Handbook of Pain ManagementDocument385 pagesOxford Handbook of Pain ManagementSalma Cortez100% (8)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Hematology 2 LaboratoryDocument11 pagesHematology 2 LaboratoryChristine BadilloNo ratings yet
- BLS MCQ CoagulationDocument4 pagesBLS MCQ CoagulationsssajiNo ratings yet
- Monograph: Pulmonary Manifestations of Systemic DiseasesDocument434 pagesMonograph: Pulmonary Manifestations of Systemic DiseasesCatherine MorrisNo ratings yet
- Hemostasis, Surgical Bleeding and Transfusion GuideDocument48 pagesHemostasis, Surgical Bleeding and Transfusion Guideaddelins100% (1)
- CoagulopathyDocument121 pagesCoagulopathyMegat Mohd Azman AdzmiNo ratings yet
- ThrombophiliaDocument37 pagesThrombophiliaapi-272740672No ratings yet
- Weaning From Mechanical Ventilation Using SBT PDFDocument29 pagesWeaning From Mechanical Ventilation Using SBT PDFEdgar Bravo Santibañez100% (1)
- Coagulopatie consum coagulare diseminataDocument6 pagesCoagulopatie consum coagulare diseminataAlex Ungureanu100% (2)
- Quick Reference Guide IAB Insertion CS300 Operation ENDocument36 pagesQuick Reference Guide IAB Insertion CS300 Operation ENCatherine MorrisNo ratings yet
- Ergo TraumaDocument7 pagesErgo TraumaCatherine MorrisNo ratings yet
- Recommendations and Guidelines: 1 - IntroductionDocument7 pagesRecommendations and Guidelines: 1 - IntroductionCatherine MorrisNo ratings yet
- JTH 14015Document4 pagesJTH 14015Catherine MorrisNo ratings yet
- Anaesthetic 09Document1 pageAnaesthetic 09Catherine MorrisNo ratings yet
- BUN - Urea CTI Sheet 714176-00QDocument6 pagesBUN - Urea CTI Sheet 714176-00Qadil shabbirNo ratings yet
- Nej Mo A 0810625Document15 pagesNej Mo A 0810625Catherine MorrisNo ratings yet
- Manejo de CoagulopatiaDocument4 pagesManejo de CoagulopatiaSMIBA MedicinaNo ratings yet
- D Krzanicki HEMSDocument39 pagesD Krzanicki HEMSCatherine MorrisNo ratings yet
- Guideline - Consent - For - Anaesthesia - 2017 - Final (1) To Be UploadedDocument16 pagesGuideline - Consent - For - Anaesthesia - 2017 - Final (1) To Be UploadedCatherine MorrisNo ratings yet
- Effects of Carbon Dioxide Pneumoperitoneum For Laparoscopic CholecystectomyDocument8 pagesEffects of Carbon Dioxide Pneumoperitoneum For Laparoscopic CholecystectomyCatherine MorrisNo ratings yet
- Habib 2009Document45 pagesHabib 2009Catherine MorrisNo ratings yet
- 2021 Curriculum For ACCS Training v1.0Document62 pages2021 Curriculum For ACCS Training v1.0Catherine MorrisNo ratings yet
- SHC Antimicrobial Prophylaxis RecommendationsDocument3 pagesSHC Antimicrobial Prophylaxis RecommendationsCatherine MorrisNo ratings yet
- Frenemies Within: An Endocarditis Case in Behçet's DiseaseDocument12 pagesFrenemies Within: An Endocarditis Case in Behçet's DiseaseCatherine MorrisNo ratings yet
- Ehra Position Paper: Europace (2020) 00, 1-48 Doi:10.1093/europace/euaa065Document48 pagesEhra Position Paper: Europace (2020) 00, 1-48 Doi:10.1093/europace/euaa065Catherine MorrisNo ratings yet
- Anaesthesia For Thoracic Surgery in Children - ParticularitiesDocument56 pagesAnaesthesia For Thoracic Surgery in Children - ParticularitiesCatherine MorrisNo ratings yet
- Wang2007 PDFDocument7 pagesWang2007 PDFCatherine MorrisNo ratings yet
- Informed Consent For Anesthesia CareDocument22 pagesInformed Consent For Anesthesia CareCatherine MorrisNo ratings yet
- 27 Regional Anaesthesia - Why PDFDocument3 pages27 Regional Anaesthesia - Why PDFCatherine MorrisNo ratings yet
- GCS Adulti-PediatricDocument1 pageGCS Adulti-PediatricCatherine MorrisNo ratings yet
- Cardiopulmonary Resuscitation in Adults and Children With Mechanical Circulatory SupportDocument20 pagesCardiopulmonary Resuscitation in Adults and Children With Mechanical Circulatory SupportCatherine MorrisNo ratings yet
- Protocolo NeumoperitoneoDocument23 pagesProtocolo Neumoperitoneomarie1690No ratings yet
- Junctional Ectopic Tachycardia in Infants and Children: Ranjit I. Kylat MD - Ricardo A. Samson MDDocument8 pagesJunctional Ectopic Tachycardia in Infants and Children: Ranjit I. Kylat MD - Ricardo A. Samson MDCatherine MorrisNo ratings yet
- Capno Handout PDFDocument57 pagesCapno Handout PDFCatherine MorrisNo ratings yet
- Capno Handout PDFDocument57 pagesCapno Handout PDFCatherine MorrisNo ratings yet
- Basic Principles of HemostasisDocument5 pagesBasic Principles of HemostasisSean Matthew100% (1)
- 29 Bleeding Tendency-4Document66 pages29 Bleeding Tendency-4Youssef Refaat RaoofNo ratings yet
- Combined HemaDocument28 pagesCombined HemaViena Mae MaglupayNo ratings yet
- Heparin Resistance - Clinical Perspectives and Management StrategiesDocument7 pagesHeparin Resistance - Clinical Perspectives and Management StrategiesRaul DoctoNo ratings yet
- HEMAREV Merged PDFDocument120 pagesHEMAREV Merged PDFMae BaechuNo ratings yet
- A Cell-Based Model of Coagulation and The Role of Factor VIIa - Blood Review 2003Document5 pagesA Cell-Based Model of Coagulation and The Role of Factor VIIa - Blood Review 2003Oscar Echeverría OrellanaNo ratings yet
- aPTT TestDocument3 pagesaPTT TestMaria VisitacionNo ratings yet
- Chapter 43 - Thrombocytopenia and ThrombocytosisDocument6 pagesChapter 43 - Thrombocytopenia and ThrombocytosisNathaniel SimNo ratings yet
- Disseminated Intravascular CoagulationDocument5 pagesDisseminated Intravascular CoagulationElenaNo ratings yet
- 1.03 Secondary HemostasisDocument8 pages1.03 Secondary HemostasisShiena ArchividoNo ratings yet
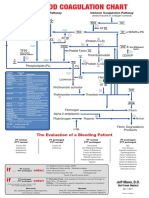
- Blood Clotting ChartDocument1 pageBlood Clotting ChartBianca SimionescuNo ratings yet
- Hemostasis and Blood CoagulationDocument9 pagesHemostasis and Blood CoagulationHans De GuzmanNo ratings yet
- Prothrombin Time (PT) PDFDocument3 pagesProthrombin Time (PT) PDFbongbongz8646100% (2)
- Costs and utilization of hemophilia patients with and without inhibitorsDocument5 pagesCosts and utilization of hemophilia patients with and without inhibitorsMelisa ClaireNo ratings yet
- Pemeriksaan Retraksi Bekuan Dan Pengukuran Masa Lisis BekuanDocument18 pagesPemeriksaan Retraksi Bekuan Dan Pengukuran Masa Lisis BekuanHery StiawanNo ratings yet
- Mechanisms of Coagulation and Fibrinolysis (Autosaved)Document60 pagesMechanisms of Coagulation and Fibrinolysis (Autosaved)Tom Anthony TonguiaNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP) Symptoms & TreatmentDocument4 pagesIdiopathic Thrombocytopenic Purpura (ITP) Symptoms & TreatmentAndrea Marie T. Artajo-BoheromNo ratings yet
- HemostasisDocument16 pagesHemostasismihikaNo ratings yet
- HemoglobinDocument15 pagesHemoglobinArya RaoNo ratings yet
- Practical Obstetric Hematology PDFDocument208 pagesPractical Obstetric Hematology PDFSteve CullenNo ratings yet
- Coagulation DisordersDocument26 pagesCoagulation DisordersLia pramita0% (1)
- Haemostasis: Case StudyDocument19 pagesHaemostasis: Case StudyTusabe FredNo ratings yet
- Blood Coagulation System Overview & Key FactorsDocument4 pagesBlood Coagulation System Overview & Key Factorsabc007200100% (1)
- Prothrombin Gene Mutation G20210A, Homocysteine, Antiphospholipid Antibodies and Other Hypercoagulable States in Ocular ThrombosisDocument5 pagesProthrombin Gene Mutation G20210A, Homocysteine, Antiphospholipid Antibodies and Other Hypercoagulable States in Ocular ThrombosisDouglas NoltieNo ratings yet