You might also like
- Coronavirus: A Guide to Understanding the Virus and What is Known So FarFrom EverandCoronavirus: A Guide to Understanding the Virus and What is Known So FarNo ratings yet
- COVID19 Health Sector Jamaica - Final - 0Document15 pagesCOVID19 Health Sector Jamaica - Final - 0Ayana ChristianNo ratings yet
- Brief2 COVID 19 Final June2020 PDFDocument19 pagesBrief2 COVID 19 Final June2020 PDFAashmeen KaurNo ratings yet
- MUN PositionpaperDocument3 pagesMUN PositionpaperchingkuoyNo ratings yet
- Progress in Disaster Science: Mikio Ishiwatari, Toshio Koike, Kenzo Hiroki, Takao Toda, Tsukasa KatsubeDocument4 pagesProgress in Disaster Science: Mikio Ishiwatari, Toshio Koike, Kenzo Hiroki, Takao Toda, Tsukasa KatsubeNicole FrancisNo ratings yet
- Maxron Holder Seventh IssueDocument14 pagesMaxron Holder Seventh IssueamandaNo ratings yet
- ACTIVITY 1 EssayDocument3 pagesACTIVITY 1 EssayMichael Enzo GeronimoNo ratings yet
- GHRP-COVID19 May UpdateDocument79 pagesGHRP-COVID19 May UpdateMohammad Ariful Hoque ShuhanNo ratings yet
- LANCET LOCKDOWN NO MORTALITY BENEFIT A Country Level Analysis Measuring The Impact of Government ActionsDocument8 pagesLANCET LOCKDOWN NO MORTALITY BENEFIT A Country Level Analysis Measuring The Impact of Government ActionsRoger EarlsNo ratings yet
- Enfermedades No Transmisibles - y Ahora Que - Lancet - 2022Document1 pageEnfermedades No Transmisibles - y Ahora Que - Lancet - 2022andrea riveraNo ratings yet
- SG Report - Advance Unedited VersionDocument23 pagesSG Report - Advance Unedited VersionJesus GabrielNo ratings yet
- Mitigating The COVID-19 Spread: A Challenge and An Opportunity Mitigar La Propagación de La COVID-19: Un Desafío y Una OportunidadDocument4 pagesMitigating The COVID-19 Spread: A Challenge and An Opportunity Mitigar La Propagación de La COVID-19: Un Desafío y Una OportunidadLuis Fernando RiosNo ratings yet
- PCX - ReportDocument16 pagesPCX - Reportgowtham thakutNo ratings yet
- PCX - ReportDocument16 pagesPCX - Reportgowtham thakutNo ratings yet
- An Astonishing News Article: I. IntroductionDocument4 pagesAn Astonishing News Article: I. IntroductionBarbatos Jr.No ratings yet
- General Assembly: United NationsDocument19 pagesGeneral Assembly: United NationsArdian SmNo ratings yet
- Containment Plan: Novel Coronavirus Disease 2019 (COVID 19)Document22 pagesContainment Plan: Novel Coronavirus Disease 2019 (COVID 19)Mayank MishraNo ratings yet
- Invasive ManagementDocument10 pagesInvasive ManagementMerazel GuadalupeNo ratings yet
- INSIGHTS DAILY CURRENT AFFAIRS PIB SUMMARY - 8 June 2020 PDFDocument19 pagesINSIGHTS DAILY CURRENT AFFAIRS PIB SUMMARY - 8 June 2020 PDFShivangi SahuNo ratings yet
- Libya Health Sector Bulletin June 2020Document21 pagesLibya Health Sector Bulletin June 2020Freedom BreezeNo ratings yet
- Manzanedo RD, Manning PDocument4 pagesManzanedo RD, Manning PmaiconNo ratings yet
- Draft ResolutionDocument6 pagesDraft Resolutionsuvendu shekhar MahakudNo ratings yet
- The Economy in The Time OF: COVID-19Document64 pagesThe Economy in The Time OF: COVID-19megabangNo ratings yet
- Papper (HOI)Document3 pagesPapper (HOI)Rizal RahmatulohNo ratings yet
- Critique Paper - CovidDocument4 pagesCritique Paper - CovidAliana CorralNo ratings yet
- Regional Report Ncds Caribbean OverviewDocument3 pagesRegional Report Ncds Caribbean OverviewBernews2No ratings yet
- Final JRSUSA Policy-BriefDocument28 pagesFinal JRSUSA Policy-BriefPrachi Tripathi 42No ratings yet
- The Economy in The Time OF: COVID-19Document64 pagesThe Economy in The Time OF: COVID-19Aristegui NoticiasNo ratings yet
- The Economy in The Time of Covid 19Document64 pagesThe Economy in The Time of Covid 19Marcelo Garcia AlmaguerNo ratings yet
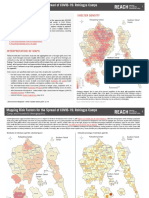
- Mapping Risk Factors For The Spread of COVID-19: Rohingya CampsDocument7 pagesMapping Risk Factors For The Spread of COVID-19: Rohingya CampsJamil SakerNo ratings yet
- Activity 3Document3 pagesActivity 3Tristan Jerald BechaydaNo ratings yet
- Afghanistan: COVID-19 Multi-Sector Humanitarian Country PlanDocument41 pagesAfghanistan: COVID-19 Multi-Sector Humanitarian Country PlanGetachew HussenNo ratings yet
- Geographies of The COVID-19 Pandemic: Reuben Rose-RedwoodDocument10 pagesGeographies of The COVID-19 Pandemic: Reuben Rose-Redwoodcarol_israelNo ratings yet
- Correspondence: What Can COVID-19 Teach Us About Responding To Climate Change?Document1 pageCorrespondence: What Can COVID-19 Teach Us About Responding To Climate Change?Aan EdisonNo ratings yet
- Communicable DiseasesDocument10 pagesCommunicable Diseases2j9hddr7kpNo ratings yet
- Containing The COVID 19 Pandemic in Nigeria A Reflection On Government Actions and Citizens ReactionsDocument8 pagesContaining The COVID 19 Pandemic in Nigeria A Reflection On Government Actions and Citizens ReactionsEditor IJTSRDNo ratings yet
- Una Narrativa Crítica de La Preparación y Respuesta de Ecuador A La Pandemia de COVID-19Document4 pagesUna Narrativa Crítica de La Preparación y Respuesta de Ecuador A La Pandemia de COVID-19Jhon LandonNo ratings yet
- Project Proposal On Health Promotion and Awareness Creation of Corona VirusDocument11 pagesProject Proposal On Health Promotion and Awareness Creation of Corona VirusNyanda DeconomyNo ratings yet
- Critical Preparedness, Readiness and Response ActionsDocument13 pagesCritical Preparedness, Readiness and Response Actionssusikaran1981No ratings yet
- Who CXB Situation Report 29Document8 pagesWho CXB Situation Report 29Zisan AhmedNo ratings yet
- 1 s2.0 S2590198220301287 MainDocument7 pages1 s2.0 S2590198220301287 MainVandemarkNo ratings yet
- Epidemiology of Public Health EmergenciesDocument11 pagesEpidemiology of Public Health EmergenciesMatti MendozaNo ratings yet
- Vaccine: Mallory Trent, Holly Seale, Abrar Ahmad Chughtai, Daniel Salmon, C. Raina MacintyreDocument8 pagesVaccine: Mallory Trent, Holly Seale, Abrar Ahmad Chughtai, Daniel Salmon, C. Raina MacintyreUsama WaheedNo ratings yet
- 1 s2.0 S0048969721038614 MainDocument12 pages1 s2.0 S0048969721038614 MainLiezl Andrea Keith CastroNo ratings yet
- BMJ n91 FullDocument4 pagesBMJ n91 FullLouise RolimNo ratings yet
- Use Only: COVID-19 Pandemic: Emerging Perspectives and Future TrendsDocument8 pagesUse Only: COVID-19 Pandemic: Emerging Perspectives and Future TrendsAmin TabishNo ratings yet
- EnvironmentDocument2 pagesEnvironmentsingh99anushka19No ratings yet
- Un-Cross-Border Human Mobility Amid and After Covid-19Document20 pagesUn-Cross-Border Human Mobility Amid and After Covid-19Jast NaufalNo ratings yet
- Contingency Planning ChecklistDocument36 pagesContingency Planning Checklistpatrickcolmenar5No ratings yet
- National Covid-19 Testing Action Plan: Pragmatic Steps To Reopen Our Workplaces and Our CommunitiesDocument30 pagesNational Covid-19 Testing Action Plan: Pragmatic Steps To Reopen Our Workplaces and Our CommunitiesChiodo72No ratings yet
- National Covid-19 Testing Action Plan: Pragmatic Steps To Reopen Our Workplaces and Our CommunitiesDocument29 pagesNational Covid-19 Testing Action Plan: Pragmatic Steps To Reopen Our Workplaces and Our CommunitiesBrank XerozeronotchNo ratings yet
- PIIS2667193X21000697Document2 pagesPIIS2667193X21000697Sara MarzoukNo ratings yet
- Transport Policy: Prathvi Thumbe Narasimha, Pradyot Ranjan Jena, Ritanjali MajhiDocument13 pagesTransport Policy: Prathvi Thumbe Narasimha, Pradyot Ranjan Jena, Ritanjali MajhiHbiba HabboubaNo ratings yet
- CDC Activities Initiatives For COVID 19 ResponseDocument60 pagesCDC Activities Initiatives For COVID 19 ResponseCNBC.com87% (23)
- Executive Board of The United Nations Development Programme, The United Nations Population Fund and The United Nations Office For Project ServicesDocument14 pagesExecutive Board of The United Nations Development Programme, The United Nations Population Fund and The United Nations Office For Project ServicesFrengkyNo ratings yet
- The Calls For International Solidarity and Transparency Toward The Combat of The COVID 19 Crisis.Document2 pagesThe Calls For International Solidarity and Transparency Toward The Combat of The COVID 19 Crisis.chingkuoyNo ratings yet
- Coronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentFrom EverandCoronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentRating: 5 out of 5 stars5/5 (1)
- Report of the Secretary-General on the Work of the Organization 2021From EverandReport of the Secretary-General on the Work of the Organization 2021No ratings yet
- Everything You Should Know About the Coronavirus: How it Spreads, Symptoms, Prevention & Treatment, What to Do if You are Sick, Travel InformationFrom EverandEverything You Should Know About the Coronavirus: How it Spreads, Symptoms, Prevention & Treatment, What to Do if You are Sick, Travel InformationNo ratings yet
- AishwaryaDocument52 pagesAishwaryamohitNo ratings yet
- STEVENS DRRR Module 6 Opon Christian Joy ADocument7 pagesSTEVENS DRRR Module 6 Opon Christian Joy AAnthony Bryan Cartujano100% (1)
- Endo Gia Curved Tip Reload With Tri StapleDocument4 pagesEndo Gia Curved Tip Reload With Tri StapleAntiGeekNo ratings yet
- Gallstone, Choledocholithiasis, Ascending CholangistisDocument12 pagesGallstone, Choledocholithiasis, Ascending CholangistisNurulasyikin MAA100% (1)
- Im9 2002 PDFDocument89 pagesIm9 2002 PDFV1QT0RNo ratings yet
- 57 2 3 BiologyDocument15 pages57 2 3 BiologyAadya SinghNo ratings yet
- Chapter 020Document59 pagesChapter 020api-263755297No ratings yet
- Playlist AssignmentDocument7 pagesPlaylist AssignmentTimothy Matthew JohnstoneNo ratings yet
- BECKER, Howard. Marihuana Use and Social ControlDocument11 pagesBECKER, Howard. Marihuana Use and Social ControlDanFernandes90No ratings yet
- Life-Long Learning Characteristics Self-Assessment: Behavioral IndicatorsDocument2 pagesLife-Long Learning Characteristics Self-Assessment: Behavioral Indicatorsapi-534534107No ratings yet
- GP Panel ClinicsDocument9 pagesGP Panel ClinicsKoh WYhowNo ratings yet
- Rafika RespitasariDocument8 pagesRafika RespitasariYeyen SatriyaniNo ratings yet
- English Conversation Discussion About AllergiesDocument3 pagesEnglish Conversation Discussion About AllergiesKevin ScottNo ratings yet
- Good Knight 420 GPatien ManualDocument30 pagesGood Knight 420 GPatien ManualJose Antonio AlcazarNo ratings yet
- The Varsity 39Document254 pagesThe Varsity 39cosmin_bloju8997No ratings yet
- Attitude of EMPLOYEES in Terms of Compliance of Health and SafetyDocument6 pagesAttitude of EMPLOYEES in Terms of Compliance of Health and SafetyJanice KimNo ratings yet
- Laminar AirflowDocument15 pagesLaminar AirflowKamran AshrafNo ratings yet
- Liver & Kidney Transplant - A5 Folder - Digital - 2022Document4 pagesLiver & Kidney Transplant - A5 Folder - Digital - 2022lakshminivas PingaliNo ratings yet
- Hypo - RT PC TrialDocument37 pagesHypo - RT PC TrialnitinNo ratings yet
- Care of The Hospitalized ChildDocument60 pagesCare of The Hospitalized ChildJSeasharkNo ratings yet
- AAP ASD Exec SummaryDocument7 pagesAAP ASD Exec SummaryCatherine AgustinNo ratings yet
- Fluoride Menace in OrissaDocument83 pagesFluoride Menace in OrissaProfessor PrabhatNo ratings yet
- ACSM - 2007 SpringDocument7 pagesACSM - 2007 SpringTeo SuciuNo ratings yet
- Nail Psoriasis Treatment Options and Management.99846Document20 pagesNail Psoriasis Treatment Options and Management.99846yuliNo ratings yet
- A 58 Year Old Client Is Admitted With A Diagnosis of Lung CancerDocument9 pagesA 58 Year Old Client Is Admitted With A Diagnosis of Lung CancerNur SanaaniNo ratings yet
- Major Neurological Syndromes PDFDocument260 pagesMajor Neurological Syndromes PDFVirlan Vasile Catalin100% (1)
- Material Safety Data Sheet: 1 Identification of SubstanceDocument5 pagesMaterial Safety Data Sheet: 1 Identification of SubstanceRey AgustinNo ratings yet
- Urbanization and HealthDocument2 pagesUrbanization and HealthsachiNo ratings yet
- Introduction To Epidemiology: The Basic Science of Public HealthDocument34 pagesIntroduction To Epidemiology: The Basic Science of Public Healthapi-19641337100% (1)
- Crisis Management and Human Behaviour Mca ApprovedDocument2 pagesCrisis Management and Human Behaviour Mca ApprovedVinil Gupta100% (1)