You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Drafting and Pleading FinalDocument57 pagesDrafting and Pleading FinalHarshdeep groverNo ratings yet
- Argha Sen ResumeDocument6 pagesArgha Sen ResumeHarshdeep groverNo ratings yet
- Aippm: AGENDA:-Discussion On India China Border SituationDocument8 pagesAippm: AGENDA:-Discussion On India China Border SituationHarshdeep groverNo ratings yet
- Affiliate Marketing Tips and TricksDocument3 pagesAffiliate Marketing Tips and TricksHarshdeep groverNo ratings yet
- Activity For Positive and Personal GrowthDocument1 pageActivity For Positive and Personal GrowthHarshdeep groverNo ratings yet
- Why India Was Called A "Golden Sparrow": 1.1. TradingDocument20 pagesWhy India Was Called A "Golden Sparrow": 1.1. TradingHarshdeep groverNo ratings yet
- B.A.LL.B. (HONS) / B.A.Ll.B. (Hons) / LL.B / BbaDocument5 pagesB.A.LL.B. (HONS) / B.A.Ll.B. (Hons) / LL.B / BbaHarshdeep groverNo ratings yet
- B.A.LL.B. (HONS) / B.A.Ll.B. (Hons) / LL.B / Bba: Asst. Prof. Chetna SharmaDocument24 pagesB.A.LL.B. (HONS) / B.A.Ll.B. (Hons) / LL.B / Bba: Asst. Prof. Chetna SharmaHarshdeep groverNo ratings yet
- Drafting Shanal JainDocument57 pagesDrafting Shanal JainHarshdeep grover0% (1)
- FUnding Requirement OnlineDocument1 pageFUnding Requirement OnlineSadu OmkarNo ratings yet
- 9 (B) Insurance Sector ReformsDocument18 pages9 (B) Insurance Sector ReformsBarkhaNo ratings yet
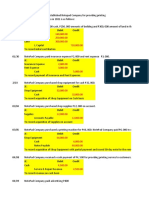
- Comprehensive Problem-Analysis of TransactionDocument43 pagesComprehensive Problem-Analysis of TransactionJoanna DandasanNo ratings yet
- Cash and Cash Equivalent QuizDocument3 pagesCash and Cash Equivalent QuizApril Rose Sobrevilla DimpoNo ratings yet
- Lesson 2 Quiz MaterialDocument4 pagesLesson 2 Quiz Materiallinkin soyNo ratings yet
- Government and Not-For-Profit Accounting Concepts and Practices 6th Edition Granof Solutions Manual DownloadDocument27 pagesGovernment and Not-For-Profit Accounting Concepts and Practices 6th Edition Granof Solutions Manual DownloadSusan Marshall100% (23)
- Zurich Captive Guide 2022Document39 pagesZurich Captive Guide 2022david.russellNo ratings yet
- Synergy Accounting Manual Guide (V5.1)Document92 pagesSynergy Accounting Manual Guide (V5.1)JM Bariani HouseNo ratings yet
- Chapter 1 & 2Document33 pagesChapter 1 & 2ENG ZI QINGNo ratings yet
- Finance and Accounting Basics - Interview Quest & Answers-1Document48 pagesFinance and Accounting Basics - Interview Quest & Answers-1naghulk1No ratings yet
- Multi-Purpose Loan Application Form (MPLAF, HQP-SLF-001, V01) EDS2Document2 pagesMulti-Purpose Loan Application Form (MPLAF, HQP-SLF-001, V01) EDS2Edelyn Lindero Ambos100% (1)
- Foreign Exchange Transaction Against RupiahDocument5 pagesForeign Exchange Transaction Against RupiahErick MulijadiNo ratings yet
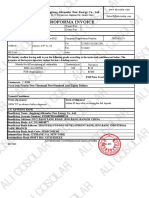
- Alicosolar Proforma Invoice For AS450WDocument1 pageAlicosolar Proforma Invoice For AS450WAngie GuerreroNo ratings yet
- Solution For Individual Assignment MCQ And14!29!14-31Document5 pagesSolution For Individual Assignment MCQ And14!29!14-31Sagita RajagukgukNo ratings yet
- PNB ChallanDocument1 pagePNB ChallanAnkana RamolaNo ratings yet
- CHAPTER 13 PPT PDFDocument90 pagesCHAPTER 13 PPT PDFMeiza AyaNo ratings yet
- William Yeboah SampongDocument62 pagesWilliam Yeboah SampongWilliam TabiNo ratings yet
- Bunna International Bank S.C Debit Card Personalization RequestDocument5 pagesBunna International Bank S.C Debit Card Personalization RequestSolomon TekalignNo ratings yet
- VM Mortgage Professional ResumeDocument2 pagesVM Mortgage Professional Resumeapi-240684563No ratings yet
- Consortium AdvancesDocument10 pagesConsortium Advancesmedhekar_renukaNo ratings yet
- Admas University College Faculty of Business Department of AccountingDocument3 pagesAdmas University College Faculty of Business Department of AccountingtemedebereNo ratings yet
- 2-Liberal Ent-PerpetualDocument2 pages2-Liberal Ent-PerpetualFroilan RolaNo ratings yet
- AmsaiDocument1 pageAmsaiDidi MiiraNo ratings yet
- Fundamentals of Accountancy, Business and Management 2: Learning Activity SheetDocument71 pagesFundamentals of Accountancy, Business and Management 2: Learning Activity SheetLeee LeeeNo ratings yet
- Jeremyybardolazacabillo: Page1of3 016palentintostbrgypansol 9 0 0 9 - 0 7 6 4 - 4 9 Calambalaguna 4 0 2 7Document4 pagesJeremyybardolazacabillo: Page1of3 016palentintostbrgypansol 9 0 0 9 - 0 7 6 4 - 4 9 Calambalaguna 4 0 2 7Jeremy CabilloNo ratings yet
- Add A New External Transfer AccountDocument1 pageAdd A New External Transfer Accountaustin OhonsiNo ratings yet
- Joint ArrangementsDocument3 pagesJoint ArrangementsCha EsguerraNo ratings yet
- Layers Egg Production Business Plan FinancialsDocument11 pagesLayers Egg Production Business Plan FinancialsTinashe RunganoNo ratings yet
- Non Performing LoansDocument11 pagesNon Performing LoansRogers256No ratings yet
- Commercial Quotation / Proposal Form: African Rand Underwriting Managers (Pty) LTDDocument6 pagesCommercial Quotation / Proposal Form: African Rand Underwriting Managers (Pty) LTDezinhleNo ratings yet